Introduction
Hibernoma is a rare, benign, and slow growing neoplasm that originates from brown adipose cells. They most commonly occur in the thigh, back, and shoulder, with less than 10% of hibernomas occurring in rare locations including the intra-abdominal region.1 Most hibernomas do not require management unless they become symptomatic and impair the patient’s quality of life. We describe a case of a rare retroperitoneal abdomino-pelvic hibernoma causing femoral nerve compression. There have been no cases of hibernoma in this location causing femoral nerve compression, with only two previous cases describing hibernoma in the thigh causing femoral nerve compression.2,3
Case Summary
A 29-year-old woman with no pre-existing medical conditions or family history of malignancy presented to the Emergency Department with sudden onset right upper quadrant epigastric pain. Her investigations and examinations in the emergency department returned as normal. After a few hours her pain improved, and she was discharged from the emergency department with an outpatient abdominal ultrasound referral. Abdominal ultrasound confirmed cholelithiasis and incidentally detected an atypical mass within the left iliac fossa measuring 10.8 x 4.9 x 6.8 cm. The mass was reported to represent a retroperitoneal lipomatous lesion with extension into the femoral canal representing a liposarcoma until proven otherwise. No abdominopelvic lymphadenopathy or metastases were identified. Urgent specialist input was requested.
The patient was reviewed in a General Surgery clinic to discuss the possibility of the mass being a liposarcoma or rhabdomyosarcoma. Due to the malignant and time-sensitive nature of these differentials, an urgent next-day positron emission computer tomography (PET CT) was scheduled, and a magnetic resonance imaging (MRI) of the abdomen and pelvis was also requested along with measurement of serum carcinoembryonic antigen (CEA) and carbohydrate antigen (CA19.9) levels. The case was also referred to for analysis and discussion at the weekly multidisciplinary team (MDT) meeting.
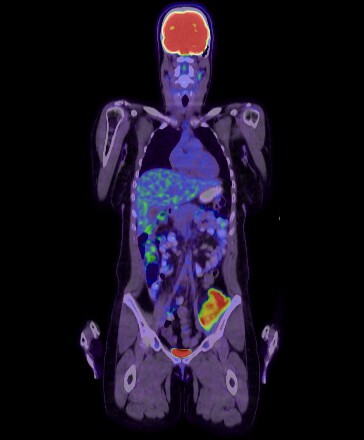
The PET/CT revealed an intensely avid lesion [standardized uptake value (SUV) max 11.4] with fat stranding in the left iliacus muscle measuring 4.9 x 6.1 x 14.6 cm (Fig. 1). No fluorodeoxyglucose (FDG) avid nodal or distant metastatic disease was reported. MRI showed a heterogeneously enhancing T2 hyperintense lesion demonstrating incomplete fat suppression in the same regions that demonstrated PET avidity. The intra-abdominal component of the left psoas musculature and the remaining musculature of the thigh demonstrated a normal appearance. Tumor markers CEA and CA19.9 were not elevated.
_and_fat_stranding_on_the_.jpeg)
CT-guided core biopsies of the left iliopsoas lesion were obtained and revealed large numbers of mature adipocytes and multivacuolated brown fat cells with a central nucleus and granular cytoplasm. No cellular atypia or mitotic activity was reported.
Immunohistochemistry revealed S100 positive cells, however no reaction was seen with SOX10, Melan A, AE1/3 or Desmin. Furthermore, no cytoplasmic granules were visualized on periodic acid-Schiff (PAS) staining. Fluorescent in-situ hybridization (FISH) testing for murine double minute 2 gene (MDM2) amplification was requested to exclude atypical lipomatous tumors/well-differentiated liposarcoma (ALT/WDS).4 FISH was performed and no amplification of the MDM2 gene (12q15) was detected. Spindle cells were not visible on histological analysis, therefore also ruling out the rare spindle cell variant of ALT/WDS.
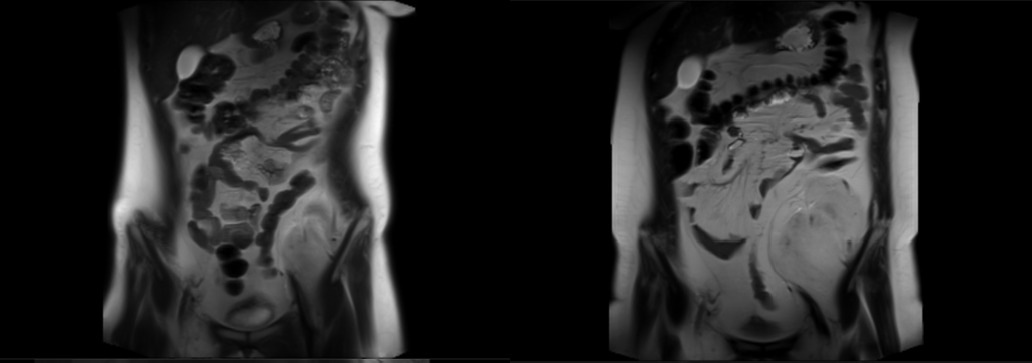
Following histological confirmation of a hibernoma, the MDT recommendation was for 6 monthly surveillance MRI scans to assess radiological and clinical progress (Fig. 2). Over the next year, two subsequent MRI scans indicated that the mass remained stable in size.
_images_depicting_the_increase_.png)
The patient had no clinical manifestations of mass effect due to the lesion, or any new constitutional symptoms.
The fourth MRI scan indicated a slow increase in size of the left iliac fossa hibernoma to 6.1 x 9.4 x 17.4 cm, including a portion of the hibernoma extending into the left inguinal region, posterior to the left common femoral vein (Fig. 2). There was also a local mass effect on the adjacent psoas muscle with displacement of bowel loops as seen in prior scans. The patient also reported new onset intermittent numbness of her left upper leg. Additionally, she did not present clinical signs and symptoms to suggest deep vein thrombosis. Due to the radiological and clinical progression of the hibernoma, a repeat core biopsy was requested to ensure no malignant change occurred.
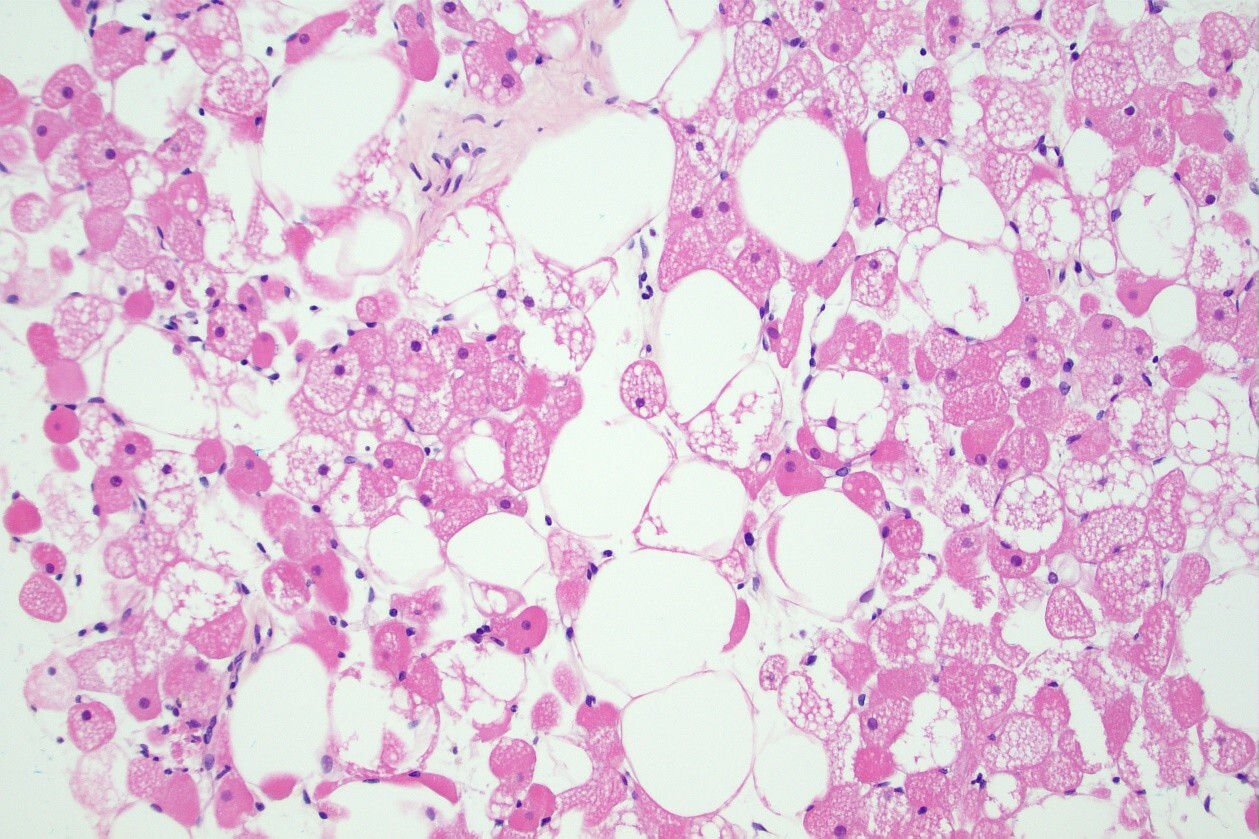
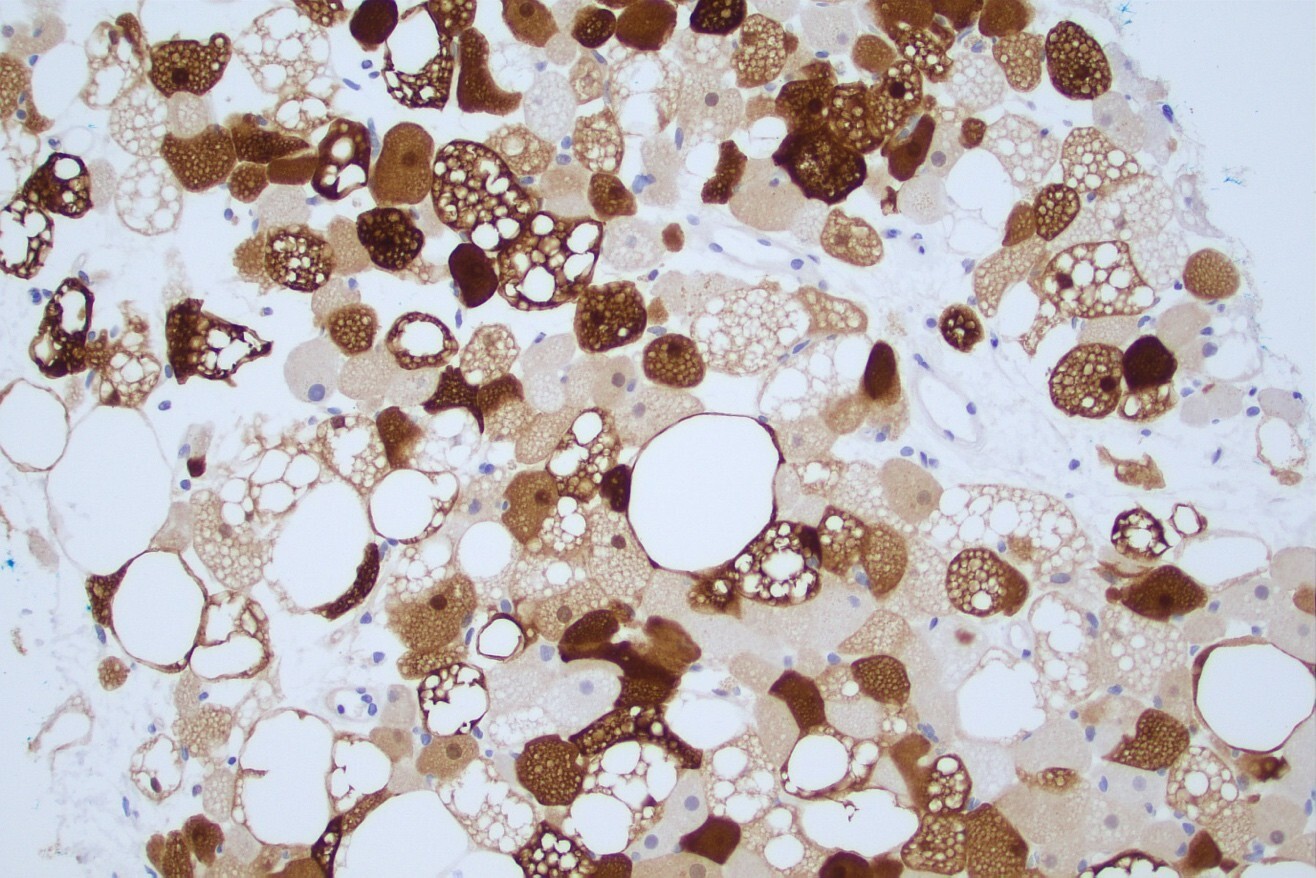
Additional CT guided biopsies were performed nearly two years and five months from the original diagnostic biopsy. These were confirmed to be adipocyte-containing lesions composed of brown adipose cells with pale-to-eosinophilic cytoplasm and univacuolated mature adipocytes (Fig. 3). Furthermore, some cells appeared multi-vacuolated and contained a granular cytoplasm (Fig. 3). No cellular atypia, mitoses, or necrosis was reported. Immunohistochemistry again revealed S100 positive cells negative for Ki67 (a commonly used proliferative marker) (Fig. 4). Thus, malignant transformation was not identified, and histological analysis of the mass confirmed the features remained consistent with hibernoma. Additionally, CT CAP indicated the left femoral nerve was stretched and showed a fat-containing lesion in the left iliopsoas musculature that was abutting the left common and external iliac vessels medially (consistent with previous imaging).
_view_of_biopsy_showing_brown_fat_cells_with_eosinophilic_granular_cytopl.jpeg)
.jpeg)
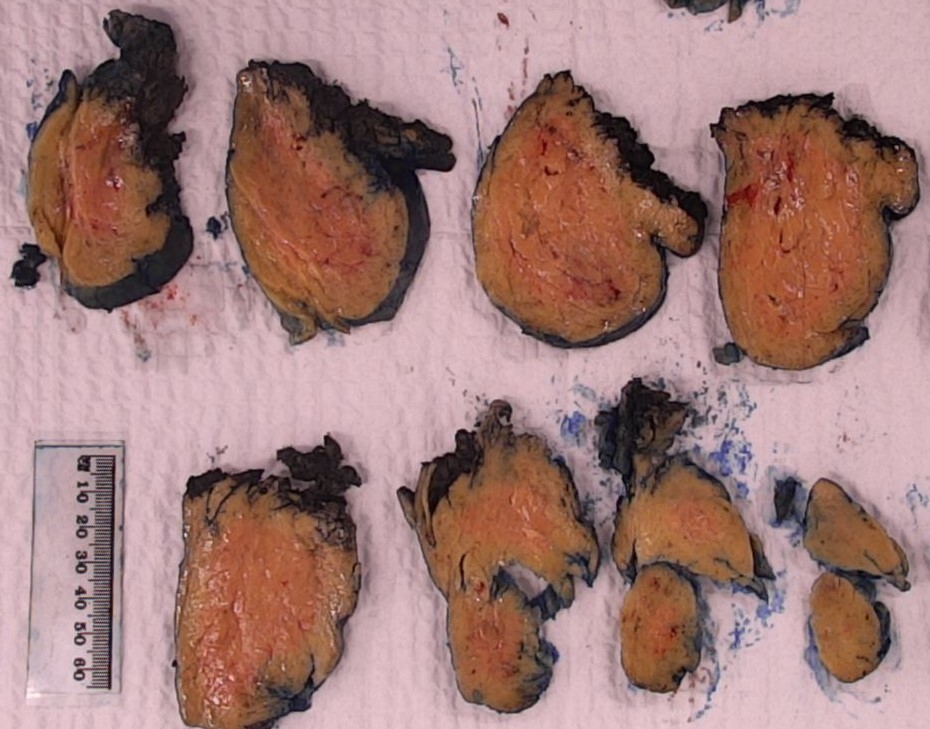
Midline laparotomy followed by mobilization of the left sigmoid colon and identification of the left ureter. The left ureter was stented intra-operatively to prevent the risk of ureteric damage. Careful efforts were made to maintain hemostasis and surgically excise the retroperitoneal hibernoma. The well-encapsulated mass was freed from the ureter and gonadal vessels. The anterior branch of the femoral nerve traversed the hibernoma laterally, and the mass was carefully bisected into two portions. The hibernoma was bisected into a medial (12.0x8.5x5.0 cm, weighing 200g) and a lateral (11.5x6.5x4.0 cm, weighing 221g) component to successfully isolate it from the femoral nerve. Both specimens contained homogenous fatty tissue with no evidence of hemorrhage or necrosis.
Microscopically, both specimens were consistent in keeping with a hibernoma (Fig. 5).

Two weeks following successful resection of the hibernoma, the patient described ongoing paresthesia of her left medial thigh that had neither improved nor worsened since the completion of surgery. Flexible cystoscopy was arranged for four weeks post-operation for removal of the left ureteric stent. No other ongoing neurological deficits were reported, and no routine follow-up was planned.
Discussion
This case is the first in the literature to report the management of a retroperitoneal pelvic hibernoma causing femoral nerve compression. Previous cases have reported femoral nerve compression only by smaller hibernomas located in the thigh.2,3 Hibernomas are well circumscribed, highly vascularized, metabolically active, and PET-avid, therefore rendering radiological differentiation from liposarcomas a challenging task. Appropriate characterization of hibernomas is achieved using a triad of clinical assessment, histological analysis, and radiological characterization. To date, there are no reports that indicate the malignant transformation of a benign hibernoma.5,6 The management of large retroperitoneal hibernomas is underreported in the literature. Retroperitoneal tumors can often grow larger in size and affect neighboring structures, thereby making surgical resection challenging. It is important to undertake a multidisciplinary team approach in managing large retroperitoneal hibernomas to ensure patient safety and successful excision.
The findings of this case report indicate that although serial imaging and monitoring remain appropriate, surgical excision remains the gold standard for definitive management of a benign hibernoma, particularly once patients report symptoms secondary to mass effect. Previous studies indicate that there is an almost negligible risk of recurrence following a successful resection.1 Despite the considerable increase in size of the hibernoma in this case, no malignant change was detected based on histological analysis pre-and post-excision.
Conclusion
Hibernomas are rare tumors that remain underreported in the literature. This case is the first in the literature to report a retroperitoneal pelvic hibernoma causing femoral nerve compression. The hibernoma was completely excised following a midline laparotomy and repeat histological analysis confirmed that the mass did not undergo any malignant change over time. We conclude that surgical excision of hibernomas, while more challenging in retroperitoneal regions such as that presented in this case, remains the gold standard of managing a hibernoma. This case report is significant for clinicians who may require guidance on the management approaches of atypical and rare hibernomas located in previously unreported locations.
Authors’ contributions
ZMN, TR, BW, SP, and PT were all involved in the collection of clinical data required for this manuscript. ZMN was responsible for case write-up, obtaining patient consent, ethics exemption, radiology and pathology images, and submission. ZMN, TR, and BW were responsible for case report write-up, literature search, and manuscript review. SP was responsible for analysis and reporting of pathological specimens. PT was the senior operating surgeon who provided advice and clinical oversight on this case.
Acknowledgements
None
Conflict of Interest
None