Introduction
Phyllodes tumours are rare fibroepithelial neoplasms of the breast, with malignant phyllodes occurring infrequently. Managing these tumours becomes more challenging when complicated by coexistence with other pathologies such as liposarcomatous differentiation and ductal carcinoma in situ (DCIS). The rarity and complexity of such cases require a nuanced understanding of diagnostic and treatment approaches.
Case Summary
A 69-year-old postmenopausal woman presented with a recently noticed lump in the left breast. Clinical examination revealed a deep-seated approximately 3 cm lump in the periareolar region at the 2 o’clock position, associated with nipple–areolar complex (NAC) retraction.
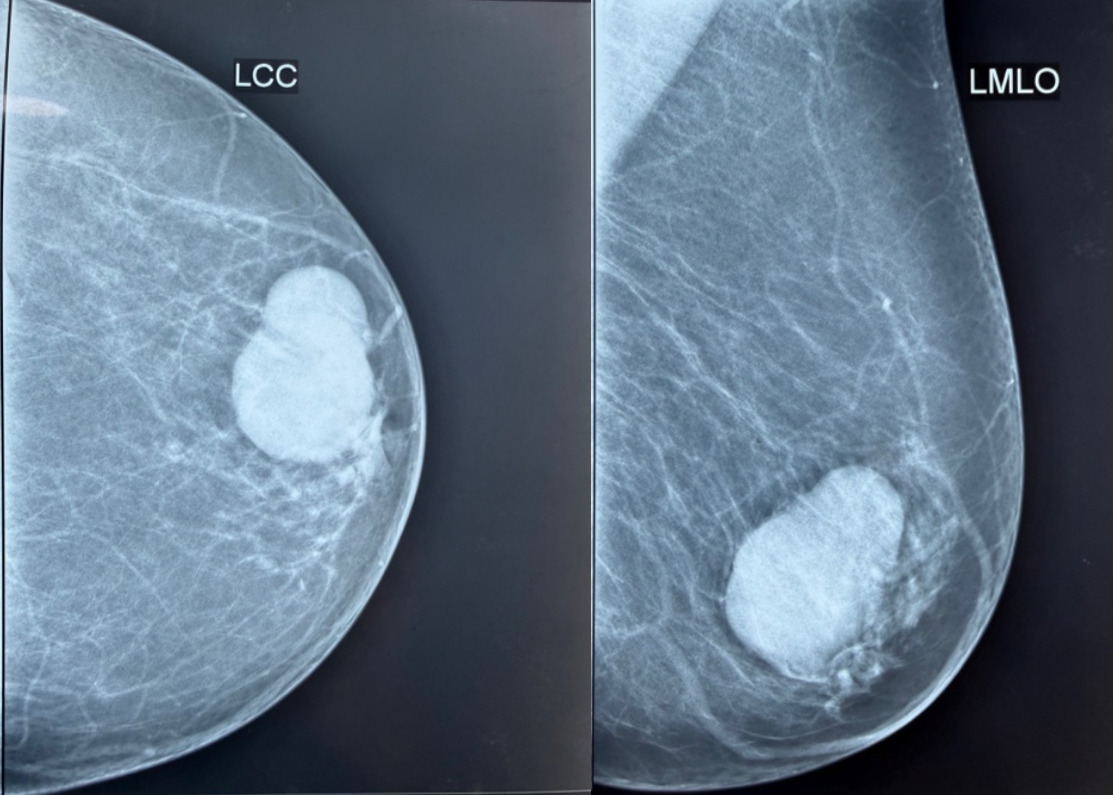
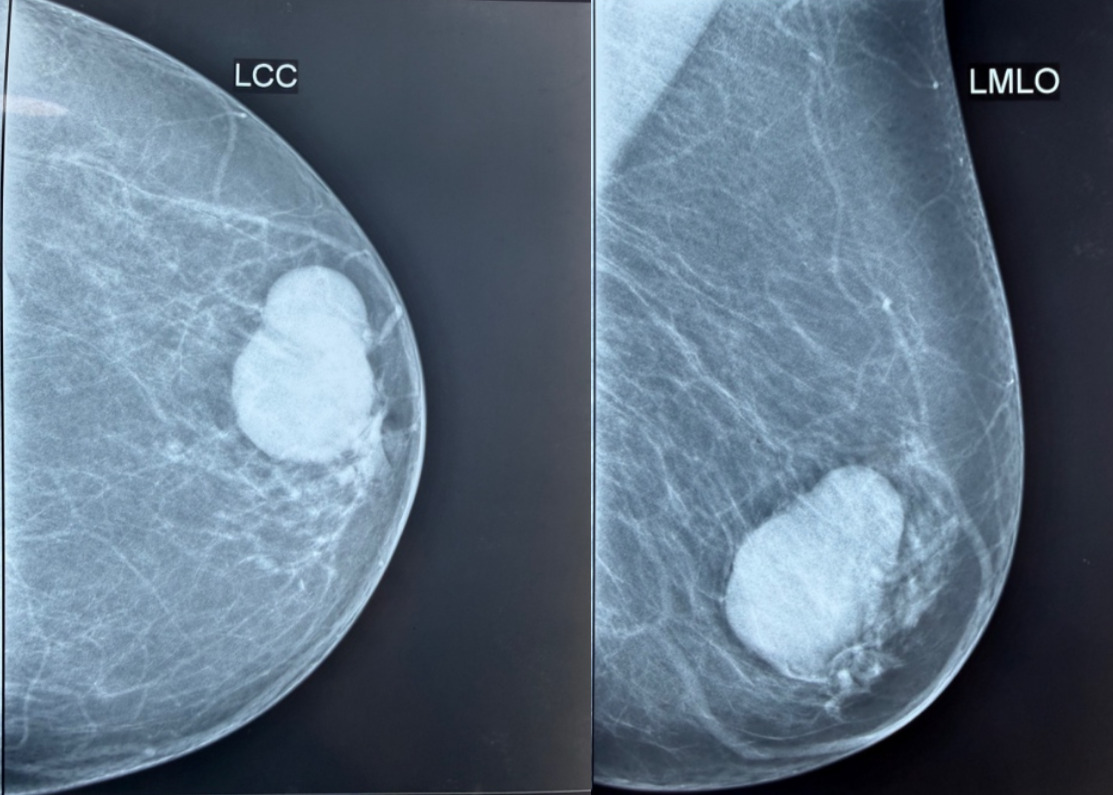
Screening mammography (Figure 1) and ultrasonography demonstrated complex cystic lesions in the left breast. One lesion measured 2.2 cm and extended from the 12 to 6 o’clock position, showing a thick-walled cyst with a solid component and floating internal debris. A second similar lesion measuring 3.6 cm was identified extending from the 10 to 3 o’clock position with mild internal vascularity. The findings were categorized as BI-RADS 4A.
Ultrasound-guided aspiration and biopsy of the solid component were subsequently performed. Cytology demonstrated acute-on-chronic inflammatory changes, while histopathological examination of the biopsied tissue suggested fibroadenoma.
A repeat breast ultrasound performed at AIG in December 2025 demonstrated interval progression to a 5.8 cm solid-cystic lesion in the upper outer quadrant of the left breast, closely abutting the nipple.
In view of the enlarging complex lesion and discordance between imaging and biopsy findings, the patient underwent wide local excision with intraoperative frozen section analysis.
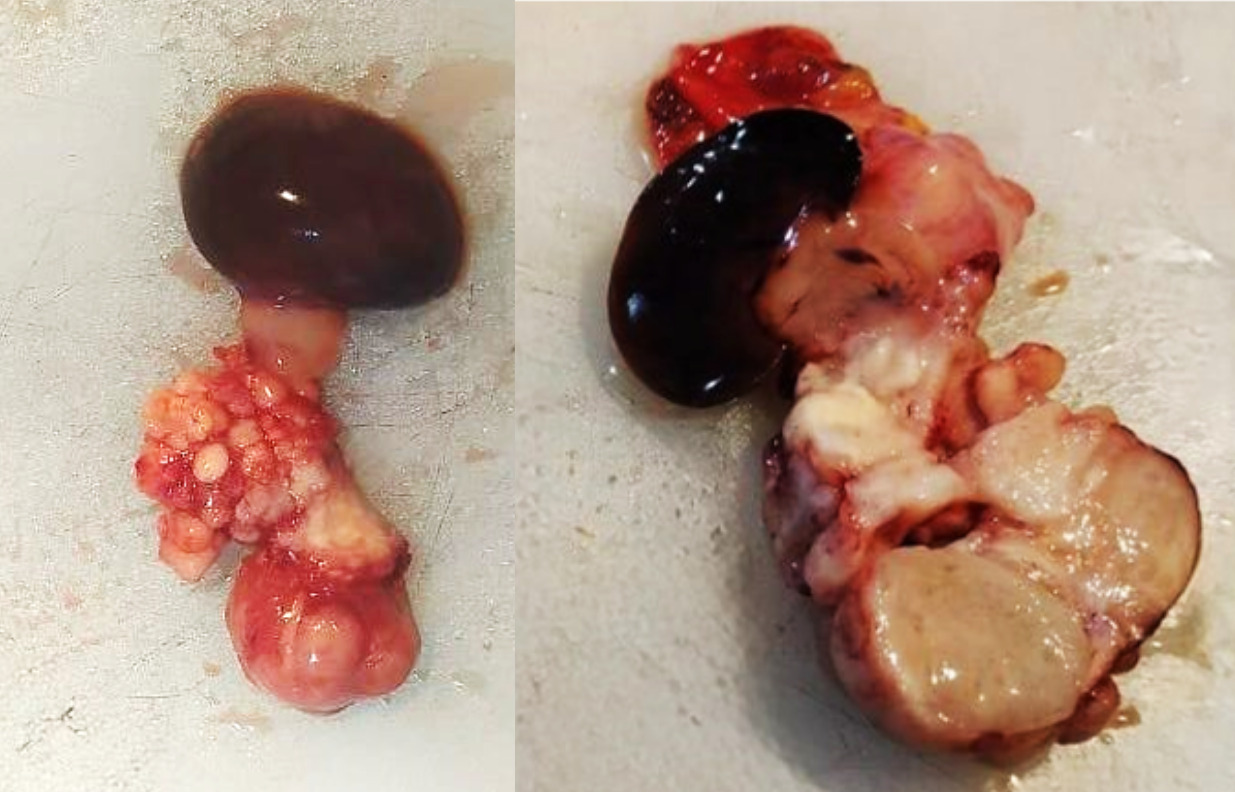
Frozen section examination revealed a biphasic tumour composed of atypical stromal elements suggestive of malignancy, along with associated ductal carcinoma in situ (DCIS). (Figure 2) No invasive epithelial malignancy was identified intraoperatively.
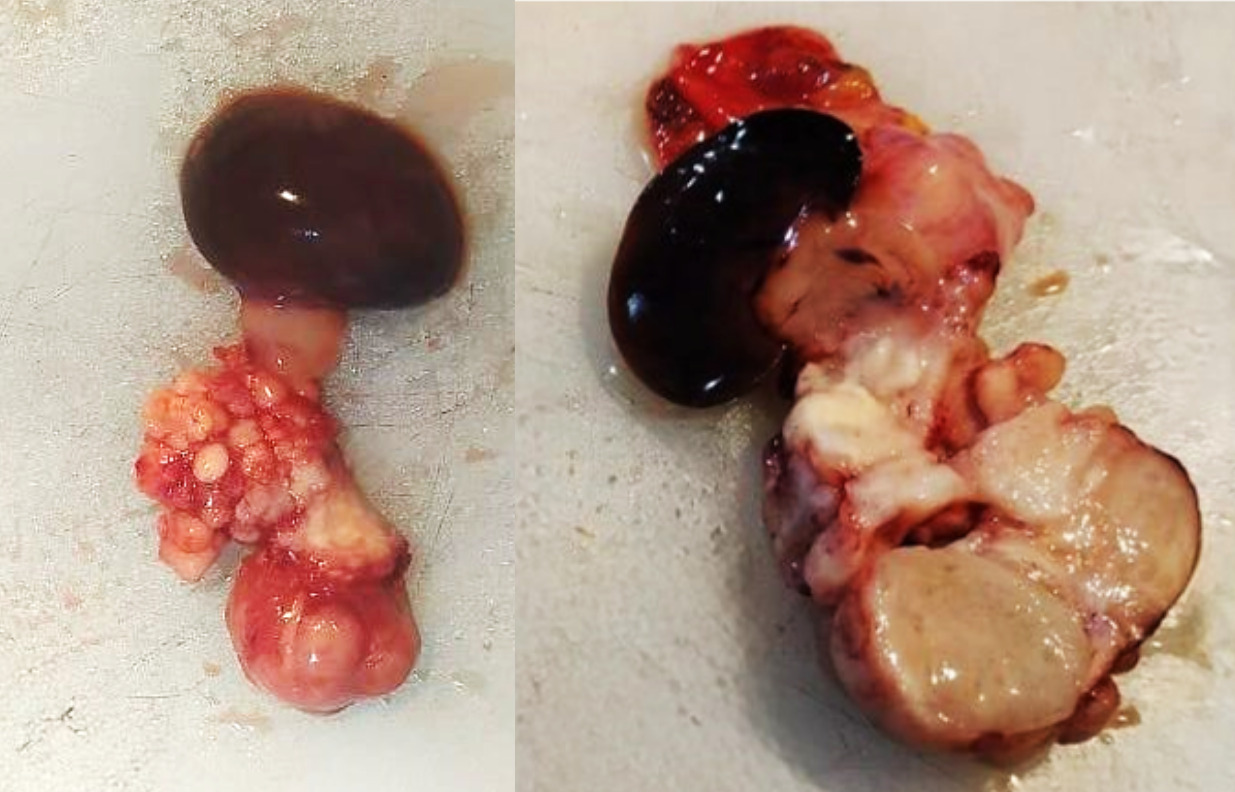
Final pathologic diagnosis was malignant phyllodes tumour with heterologous element comprising well-differentiated liposarcoma. Additional epithelial abnormalities included intermediate-grade DCIS, usual ductal hyperplasia (UDH), intraductal papilloma, and apocrine adenosis.
-
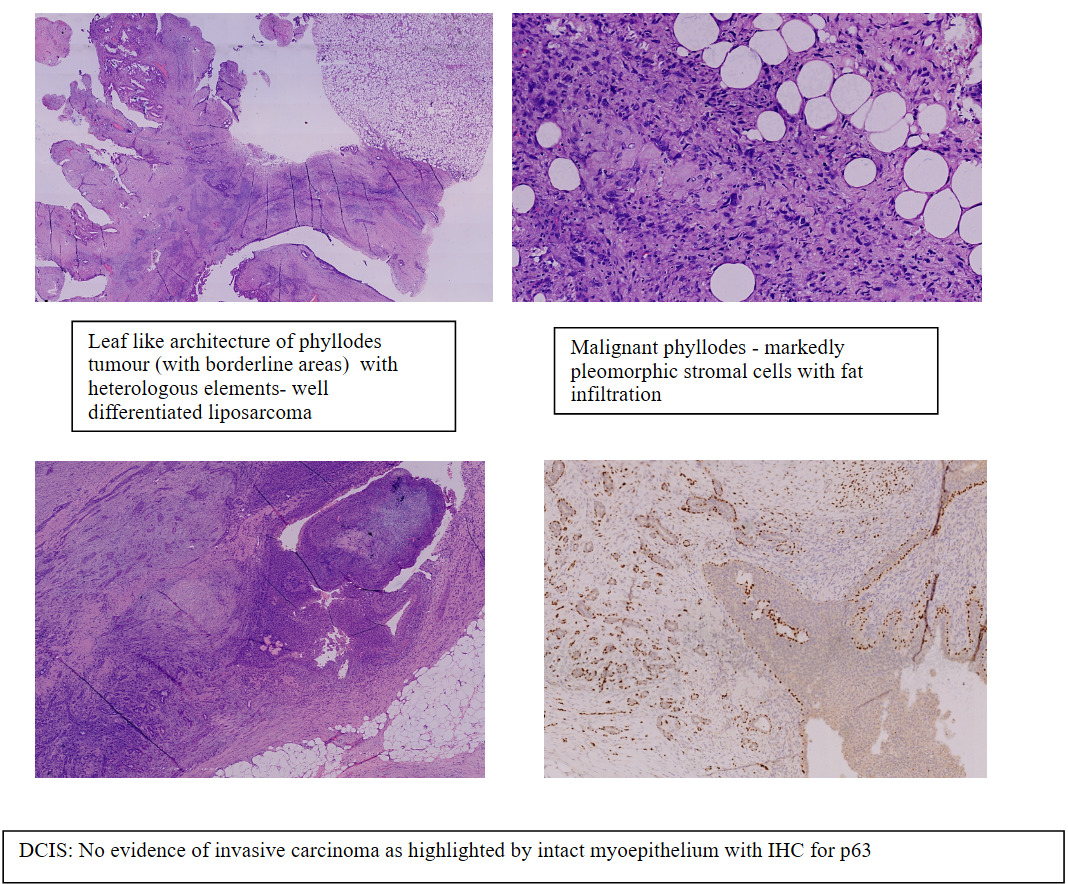
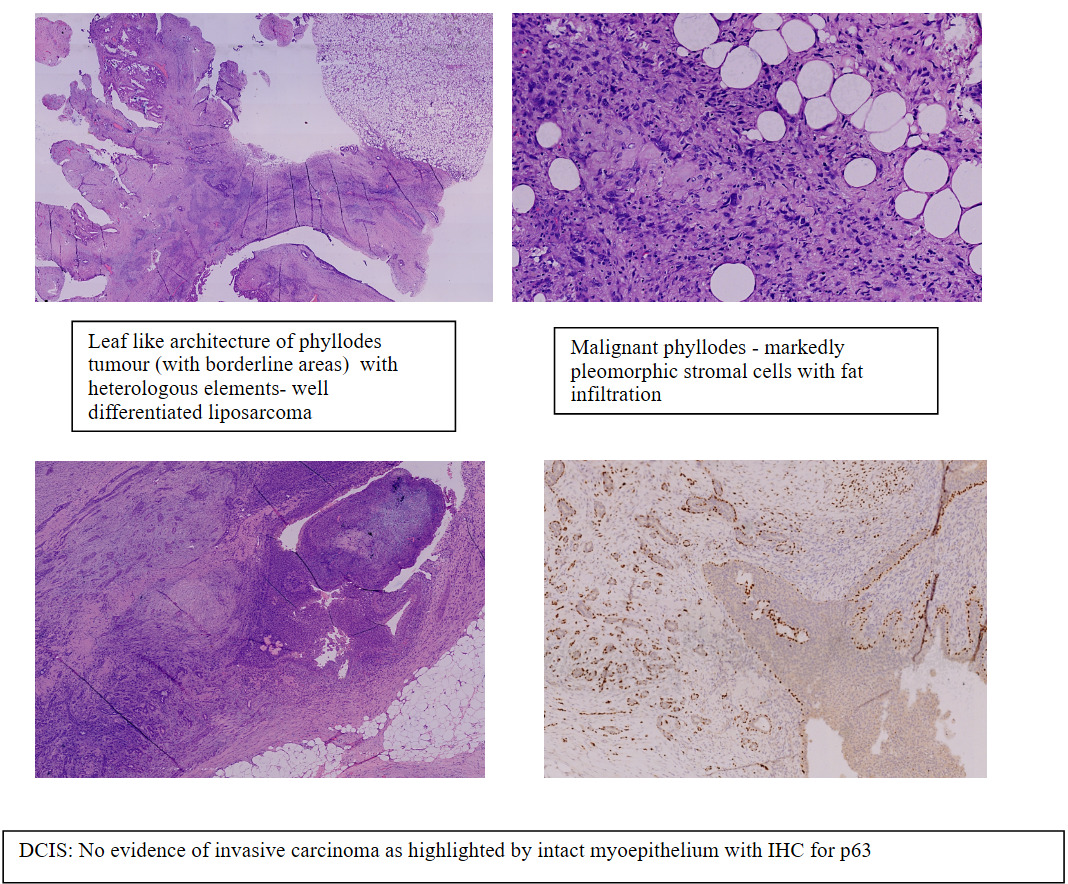
Biphasic tumour with epithelial and stromal elements, leaf like stromal fronds. Stroma variably cellular, mild to moderate cellularity resembling borderline tumour and ranging to markedly cellular areas. Stromal overgrowth with marked pleomorphic spindle cells and mitoses of 1-3/hpf. (17 mitoses per 10 high-power fields). Heterologous elements with morphology of well differentiated liposarcoma.
-
Immunohistochemistry showed patchy focal staining for smooth muscle actin (SMA) in myoepithelial cells in foci of apocrine adenosis. p63 staining in the DCIS component confirmed intact myoepithelium with no evidence of invasive carcinoma.
The Nipple areola under shave margin was free of DCIS and atypia. All surgical margins were negative.
Computed tomography of the chest performed after the surgery, did not demonstrate any evidence of intrathoracic metastasis or other abnormalities. The patient declined genetic screening.
Following multidisciplinary tumor board discussion, adjuvant radiotherapy was recommended considering the malignant phyllodes tumor, heterologous liposarcomatous differentiation, tumor size, and associated DCIS. The patient received external beam radiotherapy to the whole breast to a dose of 50 Gy in 25 fractions (2 Gy per fraction), with a simultaneous integrated boost to the tumor bed to a total dose of 57.5 Gy in 25 fractions (2.3 Gy per fraction). Tumor bed delineation was performed using surgical clips and postoperative changes with a 1 cm margin. Treatment was delivered using a five-field intensity-modulated radiotherapy (IMRT) technique with deep inspiratory breath-hold (DIBH) for cardiac sparing.
The patient tolerated treatment well and developed only grade 1 skin toxicity at the completion of radiotherapy.
This case is noteworthy for the coexistence of multiple pathological entities within a single breast lesion, including malignant phyllodes tumour, well-differentiated liposarcoma, intermediate-grade DCIS, intraductal papilloma, and apocrine adenosis. The lesion also demonstrated significant radiologic–pathologic discordance, initially mimicking a benign fibroadenoma on core biopsy.
Our report highlights the diagnostic complexity of fibroepithelial breast lesions and underscores the importance of correlating imaging, pathology, intraoperative findings, and multidisciplinary decision-making to guide appropriate management
Discussion
Phyllodes tumours (PTs) are rare fibroepithelial neoplasms accounting for approximately 0.3–1% of all breast tumours, with malignant PTs comprising only 10–20% of all cases. Their biological behaviour is largely dictated by the stromal component, where malignant transformation most commonly occurs.1,2
The present case is remarkable because of the coexistence of multiple distinct pathological entities within a single clinical presentation. What initially appeared radiologically as a complex cyst and histologically as a fibroadenoma on core biopsy ultimately revealed a malignant phyllodes tumour with heterologous liposarcomatous differentiation and an associated intermediate-grade ductal carcinoma in situ (DCIS). To our knowledge, the simultaneous presence of these five diagnostic elements within one presentation is exceedingly rare and creates a unique therapeutic challenge requiring individualized multidisciplinary management.
While distinguishing fibroadenoma from phyllodes can be made on core biopsy, often times it poses a diagnostic challenge. Features such as stromal overgrowth, atypia, cellularity, leaf like architecture and mitoses support a diagnosis of phyllodes. But all or some of these may not be seen on a core biopsy owing to tumour heterogeneity in phyllodes tumours. It is reported that fibroadenoma-like areas are seen in 35.9% of phyllodes tumours microscopically. Also at a molecular level phyllodes tumours and fibroadenomas both can harbour MED12 mutations. Pathologic findings needs to be corroborated with radiological and clinical findings in cases of discordance to facilitate optimum treatment decision.
Molecular studies have further demonstrated significant heterogeneity in PTs, with aberrations in genes such as EGFR, c-KIT and TP53, PIK3CA, RB1, NF1, PTEN, BRAF, and EGFR potentially contributing to malignant progression.3,4
Histologically, PTs are clinically classified into benign, borderline (low grade malignant), and malignant (high grade) categories based on stromal cellularity, stromal atypia, mitotic activity, stromal overgrowth, tumour border.5,6 Heterologous sarcomatous elements such as liposarcoma, osteosarcoma, and chondrosarcoma are seen in only a minority of malignant PTs.7 The presence of liposarcomatous component alone does not confer a diagnosis of malignant phyllodes.4 However in the present case the presence of stromal overgrowth along with marked atypia with abundant mitoses favoured a malignant phenotype.
Primary breast liposarcoma itself is extremely rare, accounting for approximately 2–10% of breast sarcomas.7–11 Liposarcomas may arise de novo or develop within cystosarcoma phyllodes.9 Their diagnosis can be challenging and occasionally requires expert pathological review. Prognosis is strongly influenced by histological subtype; dedifferentiated liposarcomas demonstrate aggressive behaviour and metastatic potential, whereas well-differentiated and myxoid variants generally have more favourable outcomes.10,11 In our care, a well differentiated liposarcoma would mean a good prognosis.
An additional unusual feature in our case was the coexistence of intermediate-grade DCIS within the lesion. Carcinoma arising in association with PT is distinctly uncommon, occurring in approximately 1% of cases.12 Both in situ and invasive carcinomas have been described, including invasive ductal carcinoma, invasive lobular carcinoma, DCIS, LCIS, tubular carcinoma, and squamous cell carcinoma.2,12 The etiopathogenesis of this coexistence remains unclear and continues to be an area of ongoing investigation. The clinical relevance of identifying an epithelial malignancy within PT is substantial, as it directly influences treatment planning, margin assessment, and adjuvant therapy recommendations.
This case also highlights the limitations of imaging and preoperative tissue diagnosis in complex fibroepithelial lesions. Mammography and ultrasound demonstrated a complex cystic lesion, while biopsy of the solid component suggested fibroadenoma. The absence of microcalcifications further reduced suspicion for DCIS. However, recurrent cyst refilling prompted surgical excision, which ultimately proved critical in establishing the correct diagnosis. Intraoperative frozen section identified a phyllodes tumour with a focus of DCIS, allowing immediate revision of margins and definitive surgical planning.
Management in this patient required balancing recommendations for three distinct pathologies simultaneously: malignant PT, liposarcoma, and DCIS. Traditionally, NCCN guidelines for PT advocate wide local excision with margins of at least 1 cm and no routine axillary staging.5 This differs from invasive breast carcinoma guidelines, where “no tumour on ink” is considered an adequate margin.13 Although the debate on the margins for PT (borderline and malignant) is ongoing, in our practice, a 1 cm margin is preferred for all PTs regardless of subtype, and this principle was followed in the present case.
From the DCIS perspective, achieving margins greater than 2 mm remains the accepted standard of care, and additional margin excisions were therefore performed accordingly. Furthermore, NCCN sarcoma guidelines emphasize complete surgical excision with wide margins for liposarcomatous lesions, particularly in high-grade tumours, to minimize local recurrence.14 Thus, surgical decision-making in this patient required integration of multiple oncologic principles rather than adherence to a single disease guideline.
Given the frozen section diagnosis of malignant PT with differentiation, metastatic workup with CT imaging was performed to exclude pulmonary metastases, the most common distant site of spread in sarcomatous tumours. As lymphatic dissemination is uncommon in PT and breast sarcoma, axillary surgery was avoided in the absence of clinically suspicious lymph nodes.
Following final histopathology and multidisciplinary tumour board discussion, adjuvant radiotherapy was recommended considering the malignant PT component and overall high-risk pathological profile.
Adjuvant radiotherapy in post BCS setting for Malignant phyllodes is known to reduce the risk of local recurrence particularly in large tumours (>5cm), high grade and close margins with a Hazard ratio of 0.31.15 Doses recommended for malignant phyllodes tumours are slightly higher than conventional ductal carcinomas of breast and closer to that used for soft tissue sarcomas. It is recommended that a BED, close to 90Gy would be appropriate for tumour control. We selected a conventional fractionation of 50Gy in 25 fractions with an SIB dose of 57.5Gy in 25 fractions which is equivalent to a BED of 90Gy.16The patient has completed treatment and remains on surveillance follow-up.
Conclusion
This case emphasizes the importance of maintaining a high index of suspicion in recurrent or complex cystic breast lesions, even when initial biopsy findings appear benign. More importantly, it illustrates how a single breast lesion may harbour multiple coexisting pathologies requiring individualized interpretation of overlapping surgical and oncological guidelines. The rarity of encountering five simultaneous diagnostic entities within one presentation makes this case educationally valuable for surgeons, radiologists, pathologists, and oncologists alike. It underscores the indispensable role of multidisciplinary collaboration, careful pathological evaluation, and adaptive clinical judgment in achieving optimal patient outcomes.