

Introduction
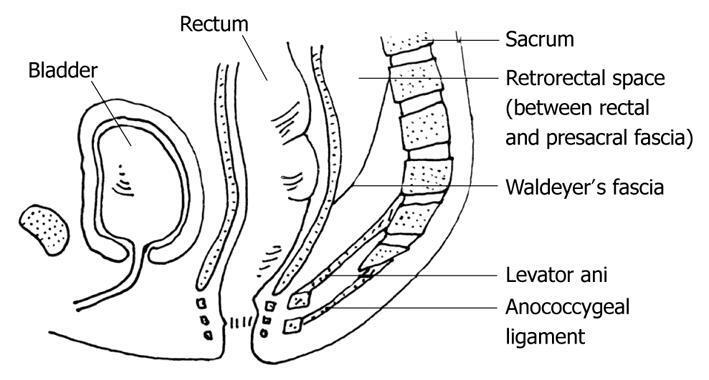
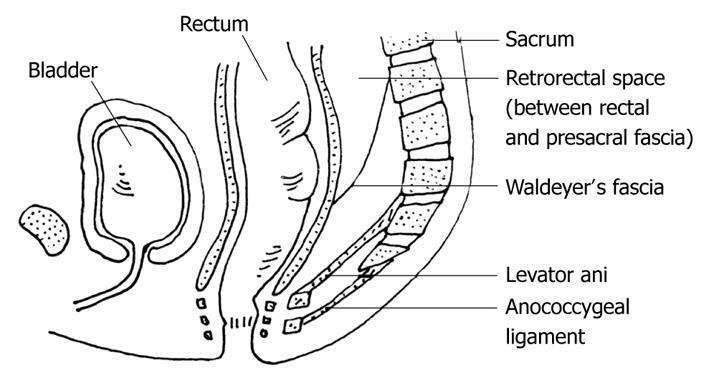
Penetrating injuries of the perineum, buttock, and gluteal region constitute a small but clinically significant category of pediatric trauma. The presacral (retrorectal) space is an anatomically complex potential space bounded anteriorly by the rectum and mesorectal fascia, posteriorly by the presacral fascia overlying the sacrum, superiorly by the peritoneal reflection of the rectosigmoid junction, inferiorly by Waldeyer’s fascia (the rectosacral fascia), and laterally by the internal iliac vascular structures and ureters.1 It is a potential space, meaning that it can accommodate significant injury—including foreign body penetration—with surprisingly limited external signs or symptoms, particularly in children who may fail to recognize or report the severity of their injury. Transgluteal impalement injuries reaching the presacral space are exceedingly rare in the pediatric literature. There is no established management algorithm, no consensus on whether bowel preparation is mandatory prior to surgical retrieval, and very limited evidence to guide surgical approach selection.
Access to this space is surgically challenging because it lies deep within the pelvis and contains delicate vascular and neural structures. Surgical approaches described in the literature include transabdominal, posterior (transsacral or parasacrococcygeal), transperineal, and transrectal techniques.1,2 The transrectal approach, which uses the method of incising the posterior rectal wall to gain access to the presacral space was employed in the present case.3
In addition to the differing surgical approaches to this space, there is a question of whether mechanical bowel preparation (MBP) is necessary. Studies have shown that no advantage is gained by pre-operative mechanical bowel preparation in elective colorectal surgery, and it can be easily avoided in order to save patients from unwanted exhaustion, distress, and adverse effects related to it.4 However, when taking a transanal approach that involves deliberate full-thickness rectal wall incision, as in transrectal presacral access, the question of bowel preparation becomes more clinically consequential.
We present the case of an 11-year-old girl who accidentally sat on a sharpened pencil concealed in her school backpack, resulting in a transgluteal impalement with a retained graphite pencil fragment in the presacral space. This case illustrates the diagnostic challenges, staged surgical decision-making, and multidisciplinary approach required to manage this uncommon injury safely, as well as the lack of a defined protocol for cases such as these.
Case Summary
An adolescent, previously healthy female presented to the emergency department after she inadvertently sat upon her backpack, which contained a freshly sharpened pencil earlier that day. She felt immediate pain in her right buttock but attributed it to her keys and continued through the remainder of her school day—including lunch and outdoor recess—before reaching back and discovering the eraser end of a pencil protruding from her right medial buttock. The patient was transferred via emergency medical services to our Emergency Department after being initially evaluated in a peripheral hospital where laboratory studies were obtained and CT imaging of the pelvis was performed. She also received IV morphine for pain, a normal saline bolus, and IV Piperacillin-Tazobactam enroute.
On arrival, the patient was awake, alert, and in no acute distress. She was positioned prone on the transport stretcher. Vital signs were all within normal limits. She reported pain rated 2 out of 10 localized to her right buttock, with no abdominal pain, rectal bleeding, or tenesmus. Physical examination was notable for approximately 1.5–2 cm of the eraser end of a yellow wooden pencil protruding from the right medial buttock without active bleeding.

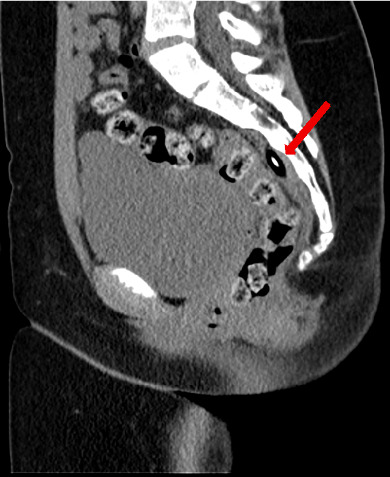
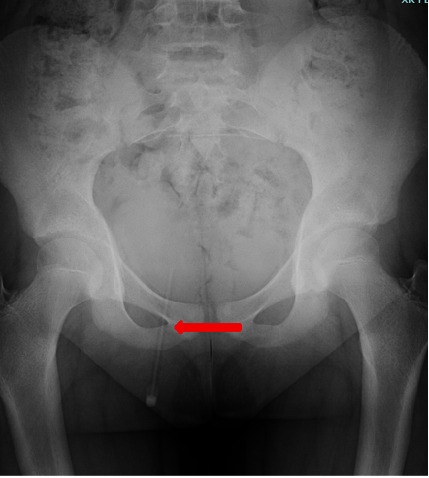
The abdomen was soft and non-tender. Neurological examination of the lower extremities was intact bilaterally. Rectal tone was normal. There was no perineal or sacral tenderness. The remainder of the examination was unremarkable. Outside CT imaging of the pelvis (without contrast) was reviewed , and imaging demonstrated a linear, pencil-shaped radiopaque foreign body with an entry wound in the medial aspect of the right gluteus. Approximately 10 cm of pencil was identified in the gluteal soft tissue and fat extending medially toward the coccyx. A break was noted at that point, with an additional 3–4 cm segment resuming in the presacral space, lying vertically between the posterior rectal wall and the sacrum, approximately 6–7 cm from the anal verge. A small associated presacral hematoma was present. No CT evidence of bowel perforation was identified.


Given the complexity of the injury—with a broken pencil producing two anatomically distinct segments—a staged surgical strategy was adopted by the trauma surgical team. The patient was taken emergently to the operating room for rectal examination under anesthesia to rule out occult rectal injury, flexible sigmoidoscopy and manual removal of the external buttock segment. The patient was positioned in left lateral decubitus position. Firm, controlled axial traction was applied to the externally visible pencil segment. A 10 cm length of wooden pencil was successfully extracted; its distal (deep) end was clearly broken, consistent with imaging. A flexible sigmoidoscopy was then performed to approximately 15–20 cm from the anal verge. The rectal vault and anal canal were unremarkable. No mucosal swelling, hematoma, intraluminal blood, perforation, or evidence of rectal injury was identified. Given the intact rectum and successful removal of the larger segment, the decision was made to defer exploration of the presacral fragment to a planned, semi-elective approach with bowel preparation. Estimated blood loss was negligible.

Following bowel preparation and around 24 hours of IV antibiotics, the patient was returned to the operating room. Digital rectal examination confirmed the retained pencil fragment palpable approximately 6–7 cm from the anal verge, lying vertically in the presacral space. An anal speculum was used to expose the posterior rectal wall. A 1 cm vertical incision was made in the posterior rectal wall directly over the palpable distal tip of the retained segment. The pencil was firmly lodged within the presacral space. A Kocher clamp was used to grasp and apply controlled traction. The fragment was retrieved in pieces but was completely removed; no palpable residual segments remained. The presacral space was copiously irrigated with normal saline followed by dilute Betadine solution. The rectal wall incision was closed in two layers using continuous 3-0 Vicryl sutures. Hemostasis was achieved. The anal canal was lightly packed with Vaseline gauze impregnated with lidocaine gel for comfort.
The patient recovered without complications. IV Piperacillin-Tazobactam was continued postoperatively for three doses. She was advanced from clear liquids to a full liquid diet and ultimately to a regular. She was discharged home in stable condition on on posteroperative day 2, with oral antibiotics (Ciprofloxacin 500 mg twice daily and Metronidazole 500 mg three times daily, both for 7 days) and bowel regimen instructions including daily Miralax to prevent constipation. The right buttock puncture wound measured approximately 0.5 cm with a clean scab at discharge. There was no surrounding erythema, warmth, or drainage. The patient pain, rectal symptoms, or constitutional complaints. The patient returned for her two-week post-discharge follow-up visit. She denied fever, pain, rectal discharge, nausea, vomiting, or altered bowel habits. Physical examination demonstrated a healing left buttock incision without erythema, warmth, or swelling. Abdominal examination was soft and non-tender with normal bowel sounds. Neurological function was intact. She was instructed to continue to avoid constipation for a minimum of one month post-injury and to follow up as needed. No further intervention was required.
Discussion
Retrorectal (presacral) space injuries from transgluteal impalement are exceptionally rare in the pediatric literature. The presacral space is a potential space bounded by loose areolar tissue, making it susceptible to foreign body migration and harboring of contaminated material with limited early symptomatology. What makes this case particularly interesting is the combination of a mundane mechanism of a child sitting on her own backpack with a highly consequential anatomical trajectory. The freshly sharpened pencil, driven by the patient’s full body weight, penetrated deeply enough to traverse the gluteal soft tissue and enter the presacral space, where it broke, leaving a segment inaccessible by simple external extraction. The initial examination was deceiving: the patient was hemodynamically stable, her abdominal exam was benign, she had no rectal bleeding, and she reported only mild pain. The child had actually attended several school classes, gone to recess, and eaten lunch with the pencil embedded in her buttock for over an hour before recognizing it.
There are multiple approaches to the retrorectal space cited in the literature. The anterior transabdominal approach is preferred for lesions at or above S3, offering excellent visualization of major pelvic vasculature and the ureters, but requires laparotomy or laparoscopy and carries greater systemic morbidity.2,5 The posterior approach—most classically the Kraske procedure—is performed prone in a jack-knife position via a parasacral or transsacrococcygeal incision and is favored for low-lying pathology below S3.6 For the lowest-lying pathology, two additional minimally invasive options exist. The perineal approach uses a para-anal skin incision to enter the retrorectal fat plane by blunt dissection between the posterior rectal wall and the presacral fascia, avoiding laparotomy entirely while preserving the sphincter complex, though it carries risks of inadvertent rectal perforation during posterior wall dissection and wound infection given the proximity to the perineum.3 The transrectal approach—incising the posterior rectal wall to gain direct access to the presacral space—represents a fourth, less commonly described method applicable specifically to low-lying pathology.3 While it deliberately violates the rectal wall, this approach avoids external incisions entirely, offers the shortest operative time, and is associated with low morbidity when the rectal wall is repaired and bowel preparation has been performed.3,7
The decision to stage the operative intervention was a critical element of this case’s successful management. On the night of presentation, the priorities were to: (1) rule out rectal perforation, which might mandate emergent bowel diversion, and (2) remove the larger, externally accessible segment. With the rectum confirmed intact by sigmoidoscopy, a semi-elective approach with proper bowel preparation became feasible and optimal. The 24-hour interval allowed mechanical cleansing of the bowel and continuation of IV antibiotics, reducing the bacterial load and contamination risk substantially for the second procedure. In this case, the transrectal route was selected given the favorable position of the fragment (6–7 cm from the anal verge) and the intact rectal wall confirmed at the first operation.
Guidelines for transanal minimally invasive surgery (TAMIS) specifically recommend that mechanical bowel preparation be administered preoperatively alongside prophylactic antibiotics, reflecting the higher stakes of controlled rectal wall transgression requiring reliable primary closure in an adequately decontaminated field.8 Broad-spectrum antibiotic coverage bridging gram-negative organisms and anaerobes is essential for presacral injuries given the proximity to rectal flora to reduce the risk of wound infection, presacral abscess, or bacteremia.
Conclusion
We have presented a case of accidental transgluteal pencil impalement in an 11-year-old girl resulting in a retained presacral foreign body with an intact rectum. This case demonstrates that low-energy, seemingly inconsequential mechanisms of injury can produce serious and anatomically complex penetrating injuries in children. Emergent sigmoidoscopy and partial foreign body removal on the night of presentation, combined with planned transrectal presacral retrieval after bowel preparation, resulted in complete foreign body removal, no infectious complications, and an uneventful recovery. This case should raise clinical awareness of the importance of thorough imaging and surgical evaluation of all pediatric perineal and gluteal penetrating injuries regardless of apparent mechanism severity or initial symptom burden. The presacral space can harbor significant injury in a deceptively stable-appearing patient, and early identification with appropriate multidisciplinary management is essential to achieving an excellent outcome.