

INTRODUCTION
Skin adnexal adenocarcinomas are exceedingly rare and aggressive malignancies originating from the adnexal structures of the skin, including hair follicles, sebaceous glands, and sweat glands. Among these, apocrine adenocarcinomas are particularly uncommon, with most cases being diagnosed only after histopathological examination. As per SEER (Surveillance, Epidemiology, and End Results) database for the USA and RARECARENET database for Europe, the overall incidence of 2.2 - 7 cases per 1 million cases annually, placing them among the rarest cutaneous malignancies.1
Apocrine adenocarcinomas can present with varied clinical features, often mimicking benign conditions such as cysts, carbuncles, or even localized infections.2 These tumors most commonly arise in areas with a high density of apocrine glands, including the axilla, anogenital region, and scalp. Clinically, they present as slow-growing, painless nodules, which may ulcerate, bleed, or produce a foul odor as they progress, as was seen in the current case. Given their subtle presentation, early diagnosis is often missed, leading to delayed treatment.
Histopathological confirmation is crucial in distinguishing skin adnexal adenocarcinomas from other cutaneous malignancies, particularly squamous cell carcinoma and metastatic adenocarcinoma from internal organs.3 Immunohistochemistry (IHC) markers, including CK7, GATA3, and P63, are commonly used to confirm the adnexal origin of the tumor and exclude other malignancies.3
The prognosis for patients with skin adnexal adenocarcinoma is generally poor, especially in cases where there is lymphatic or distant metastasis. Surgical resection with clear margins remains the cornerstone of treatment; however, there is no consensus on the optimal margin width or the use of adjuvant therapies, such as radiation and chemotherapy. Guidelines for the management of these tumors are lacking due to their rarity, leading clinicians to adopt strategies from the treatment of more common skin malignancies such as soft tissue sarcomas and squamous cell carcinomas.4
This report highlights a rare case of apocrine skin adnexal adenocarcinoma in the pubic region of a 49-year-old male, outlining the diagnostic challenges, clinical course, and treatment strategies. It also underscores the importance of a multidisciplinary approach in managing such complex and aggressive tumors.
CASE PRESENTATION
Patient Details
RM is a 49-year-old male with chief complaint of rapidly growing mass in the pubic area. He initially noticed a painless, pimple-like lesion in the pubic region approximately six weeks prior to consultation. Over time, the lesion increased in size, developed a foul odor, and eventually became painful. Eventually minimal purulent discharge with some blood oozing from the more friable portions of the lesion was noted. Then around two weeks prior to consultation, the patient experienced difficulty ambulating due to discomfort from the size of the mass. At this point, no consultation was done and the rapidly growing mass was only known to the patient.
Now one week prior, the patient noted the beginning of a non healing wound on the sole of the right foot, their initial reason for consultation. During admission in the Emergency Room, the pubic mass was now discovered, hence the one given more attention and management.
His personal and social history is unremarkable. He is an office employee, with no exposure to radiation or chemicals. On probing his sexual history, the patient has a total of two non-simultaneous sexual partners and claims to have no sexual activity for at least six weeks prior to his consultation.
On focused physical examination, the patient has a pubic mass measuring 15 x 12 cm friable, foul-smelling mass with purulent discharge and macerated skin edge. Additionally, the patient’s foot lesion measured 1.5 x 1.5 cm open wound located on the sole of the right foot, no active bleeding, no tenderness surrounding the lesion.
_upon_arrival_at_the_er__(b)_after_one_week_of_wet-to-dr.jpeg)
Diagnostic Assessment
Diagnostics done included CBC which showed leukocytosis (WBC 16.8), increased neutrophils (82%), and thrombocytosis (Plt 458). Abdominopelvic CT scan showed an enhancing fungating soft tissue mass measuring about 7.3 x 12.6 x 9.6 cm (AP x W x CC) seen in the skin of the mid anterior lower abdominal region extending inferiorly to the left inguinal area with associated underlying minimal subcutaneous fat stranding. While MRI showed a lobulated fungating enhancing cutaneous mass corresponding to the CT findings.
_axial_on_pd_phase_(b)_axial_on_t1_phase_(.jpeg)
Preoperative Plan
Upon admission, the patient was already primed for surgical intervention. Wedge biopsy was immediately done to determine etiology of the mass. Other pre-operative preparations include administration of IV antibiotics and wound care. In addition, bacterial culture of the wound bed was obtained in preparation for the planned split thickness skin grafting.
Therapeutic Intervention
During the patient’s admission, he was operated on a total of three times. The first procedure was an en-bloc resection of the whole tumor. Histopathology revealed infiltration of pagetoid cells hence re-excision of margins was done. The wound was initially covered with wet to dry dressing until culture results were negative and ready for split thickness skin grafting.
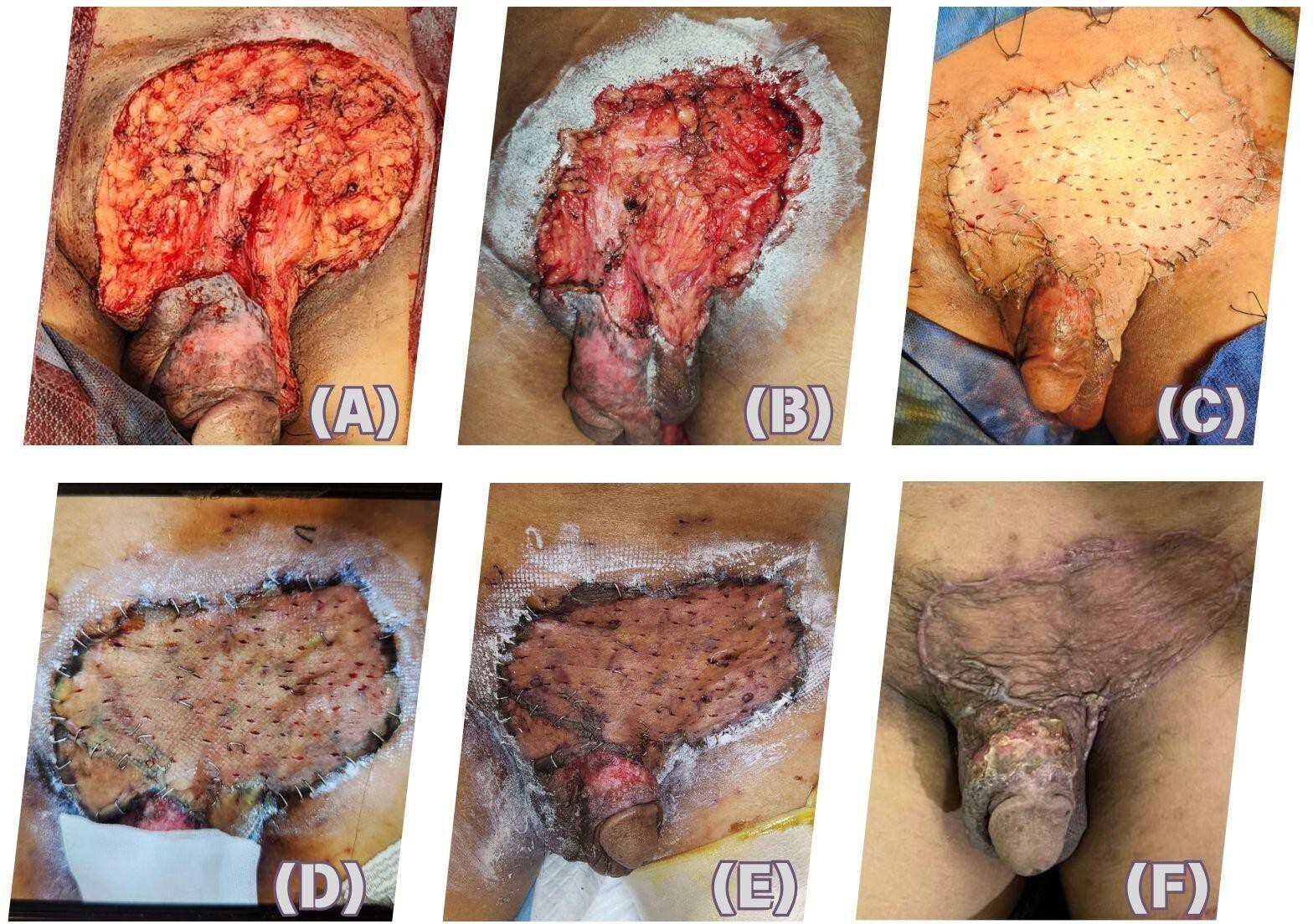
Surgical technique
Initial procedure includes a wide resection of the exophytic tumor on the pubic area ensuring a 1 cm margin from the induration of the irregularly shaped mass. Re-excision of margins was done prior to the planned reconstruction. The patient/*underwent split thickness skin grafting with careful and strategic placement of the skin graft was done to ensure adequate coverage for the complex shape of the defect. Summary of the surgical technique can be seen in Figure 3.
Intraoperative findings
During the first procedure, there was note of a 13x12x2cm firm but friable irregularly shaped mass with foul smell in the pubic area. Which was then reduced to approximately a 10 x 11 cm wound cavity. The third procedure was only done when there was note of good granulation tissue, pink and viable wound bed for the graft. As for the plantar area of the left foot, 1.5 x 1.5 cm open wound, adjacent to hyperpigmented lesion on the plantar aspect of the left foot. This eventually developed scar from the incision done.
_after_wide_resection__(b)_after_plastic_tackin.jpeg)
Follow up and Outcomes
On follow up with Plastics, there was good uptake of the flap, there was just some dryness on a small portion of the shaft of the penis but resolved with moisturizer. This was not problematic for the patient. However, in the interim, the patient had sudden onset weakness on bilateral lower extremities, initially this was managed by Orthopedics department. where conservative management was done and the patient was advised exercises there was now note of bone metastasis in a short span of time as evidenced by the CT scan findings of multiple predominantly lytic
lesions involving the imaged vertebrae, and the adjacent osseous structures, to varying levels. Pertinent findings include the ff:
-
Collapse of most of the T1-T5 vertebral body heights, most notably involving the T1 (by 75% relative to C7) and T5 (by 67% relative to T6)
-
Expansile lytic lesions with soft tissue components which involve the following: Spinous process of C5 and right pedicle of C6; Right transverse process of C7, with possible involvement of the corresponding
right transverse foramen; Right laminae, articulating processes, and proximal portions of the right posterior ribs of levels T1 to T3, with neuroforaminal expansion and involvement of the spinal cord at these levels by the soft tissue components.
-
Rightward deviation of the spine is also evident at this level.
-
Lytic changes also involve the left pedicle and hemivertebra of T12, with 21% decreased vertebral body height by relative to its right counterpart
The patient underwent spine surgery where biopsy of the lesions were taken showing malignant round cell neoplasm favoring metastasis. And due to the turn of events and the life changing impact that the condition has caused, the patient was also referred to Psychiatry for treatment of his adjustment disorder.
Histopathology Results
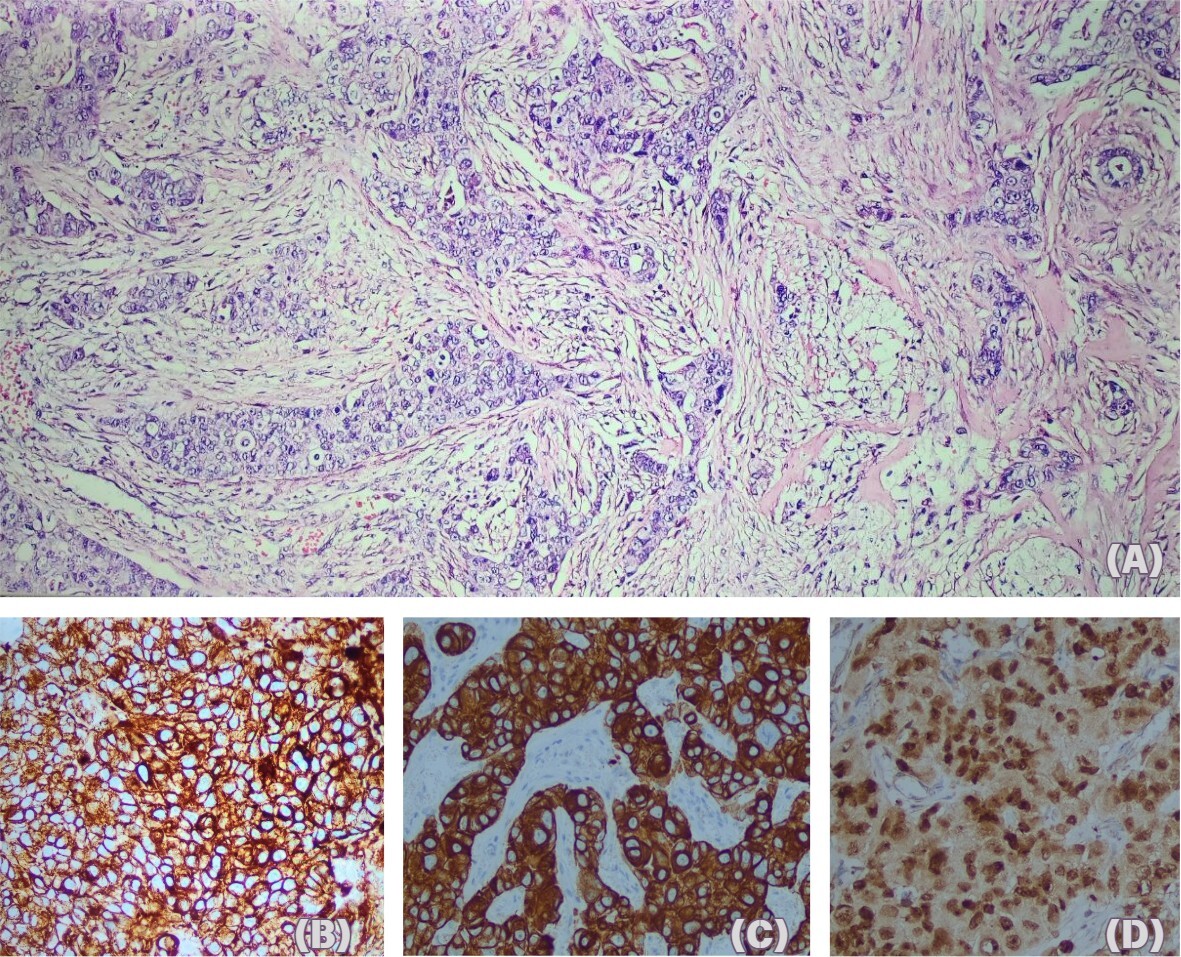
_poorly_differentiated_carcinoma_favori.jpeg)
Initially seen as a poorly differentiated carcinoma favoring squamous cell carcinoma, additional IHCs now shifted and narrowed down the differentials. In summary of all the immunohistochemistry staining done the presence of CK7 and GATA-3 positivity points us to three possibilities of a carcinoma of (1) the breast, (2) skin adnexa, and (3) urothelial primary however the positive focal staining for p63 and CK5/6 tells us that urothelial and skin adnexal carcinomas less likely differentials. With this further IHC and additional imaging work up were done to confirm a breast primary - breast sonogram and mammogram were unremarkable. Along with this, additional IHCs reveal AR and GCPDF-15 positivity favor a malignant skin adnexal tumor with apocrine differentiation rather than a breast primary.
DISCUSSION
Cutaneous adnexal adenocarcinomas, particularly those of apocrine origin, remain a rare and challenging malignancy. These tumors arise from the adnexal structures of the skin, including hair follicles, sebaceous glands, and sweat glands, with a wide range of clinical presentations and prognoses. The rarity of these tumors poses a diagnostic challenge, often leading to delays in detection and treatment.1
A large body of literature has emphasized the importance of immunohistochemistry (IHC) in diagnosing these tumors due to their overlapping features with other skin malignancies. Markers such as CK7, GATA3, and p63, which were used in this case, are crucial in confirming the adnexal origin and distinguishing the tumor from more common cancers like squamous cell carcinoma or metastatic adenocarcinoma from the breast or gastrointestinal tract.3 The use of these markers, particularly in conjunction with clinical findings, helps narrow the diagnosis and guide appropriate treatment strategies.
The prognosis for skin adnexal adenocarcinomas, as evidenced by this case, is generally poor when diagnosed at an advanced stage, especially with lymph node involvement or distant metastases. Data from the Surveillance, Epidemiology, and End Results (SEER) and RARECARENET databases indicate that these tumors are ultra-rare, with an incidence of less than 1 per 100,000,000 annually. Their rarity has made it difficult to establish clear treatment guidelines, forcing clinicians to extrapolate from other skin cancers such as soft tissue sarcomas and squamous cell carcinomas.1
Management is primarily surgical, with wide local excision being the cornerstone of treatment. Achieving negative margins is essential, as local recurrence is common. In this case, the patient underwent multiple surgical resections, with split-thickness skin grafting to repair the defect. However, even with aggressive surgical treatment, lymphatic spread and eventual bone metastases were detected, highlighting the aggressive nature of the disease.
Adjuvant therapies, including radiation and chemotherapy, are considered in cases of advanced or recurrent disease. While there is no standardized chemotherapy regimen for skin adnexal carcinomas, protocols borrowed from other aggressive skin cancers, including taxanes, platinum-based therapies, and anthracyclines, have shown some success in cases with metastatic spread.2
The role of radiation therapy is typically adjunctive, used either to palliate symptoms or in cases of unresectable disease. In this case, the patient was initially scheduled for radiation therapy but was rejected due to complications related to the lesion’s location and the thin skin of the penis. This highlights the difficulty in managing such tumors when they invade sensitive or complex anatomical areas.
Given the ultra-rare nature of this tumor, long-term prognosis remains uncertain. Most data suggest a poor outcome when distant metastases are present, especially when there is bone involvement, as seen in this case. Long-term surveillance and systemic treatment are necessary to manage disease progression, although treatment remains largely palliative at this stage.4
CONCLUSION
This case of skin adnexal adenocarcinoma of apocrine origin illustrates the diagnostic challenges posed by rare cutaneous malignancies. The rarity of these tumors, combined with their often indolent but sometimes aggressive nature, makes early diagnosis difficult. With this, the use of immunohistochemistry is critical in confirming the diagnosis and differentiating from other more common malignancies. In terms of treatment and management of condition, surgical resection remains the mainstay of treatment, specifically with wide local excision to achieve negative margins. However, the role of adjuvant therapies, including radiation and chemotherapy, is less clear due to the absence of standardized treatment protocols.
This case then underscores the need for a multidisciplinary approach, combining surgery, pathology, and oncology to manage such complex tumors. The poor prognosis, particularly with metastatic spread, highlights the importance of early detection and individualized treatment plans. Further studies are necessary to develop specific guidelines for the diagnosis and management of skin adnexal carcinomas, particularly that of apocrine origin, more so in the context of metastatic disease.