
Introduction
Injectable aesthetic procedures such as dermal fillers for anti-aging, volume augmentation and wrinkle reduction have gained significant popularity worldwide.1 With rising demand, limited regulations and guidelines, complications—though rare—are becoming increasingly prevalent.1 There are many different types of dermal fillers including: hyaluronic acid (HA), calcium hydroxylapatite, poly-lactic acid derivatives (PLA), polymethyl-methacrylate microspheres (PMMA), collagen, and autologous fat.2 Dermal fillers such as calcium hydroxylapatite and poly-L-lactic acid (PLLA) are even able to function as biostimulators, inducing a controlled inflammatory response that stimulates fibroblasts which promotes collagen synthesis.2,3
PLA is a synthetic biocompatible and biodegradable aliphatic polyester derived from natural starches.4 Lactic acid is then polymerised into 4 sub-types: poly-D-lactic acid (PDLA), PLLA, poly-D,L-lactic acid (PDLLA), and mesoPLA.4 PDLLA is a type of stimulatory subdermal filler that was first approved in 2014 by the Korean Food and Drug Administration.5 It has been increasingly used as a cosmetic filler given its long-lasting effect and safety profile.5 Compared to HA, PDLLA lasts longer in tissues and is known for its ability to stimulate collagen by activating fibroblasts.2,3 This leads to gradual volume restoration and is claimed to promote skin rejuvenation and a more natural aesthetic result.2,3
Adverse effects of facial fillers range from mild - swelling, bruising, pain, livedo reticularis, allergic reactions, granulomas, fibrosis - to major complications such as infections, vascular occlusions, tissue necrosis, blindness, stroke and death.6 One of the most feared being vision loss due to occlusion of the ophthalmic or central retinal artery.
Case Summary
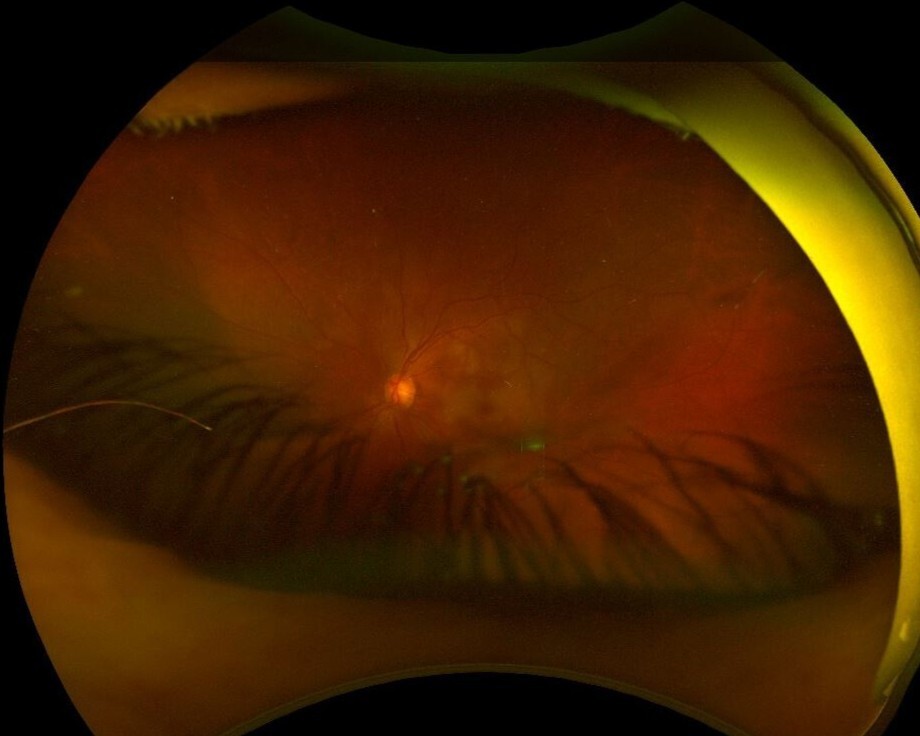
55-year-old female presented to an ophthalmologist with sudden vision loss in her left eye following self-injection of cosmetic filler to both lower eyelids and infraorbital areas. She had injected PDLLA subdermal filler (AestheFill; REGEN Biotech, Inc., Seoul, South Korea) four hours prior and reported immediate painless vision loss in her left eye following injection. On examination, best-corrected Snellen visual acuity (BCVA) in the right eye was 6/9 and in the left eye was count fingers (CF) at 1 meter. Intraocular pressure (IOP) was normal bilaterally. As seen in Figure 1, periorbital oedema and ecchymosis with mild left blepharoptosis were evident. Pupils were equal and reactive with a dense left relative afferent pupillary defect (RAPD). Extraocular eye movements were preserved. There was mild conjunctival hyperemia, a clear cornea, quiet anterior chamber and a moderate cataract. On dilated fundoscopy, as seen in the ultra-wide field fundus image in Figure 2, findings were consistent with a central retinal artery occlusion with multi-territory macular ischemia.
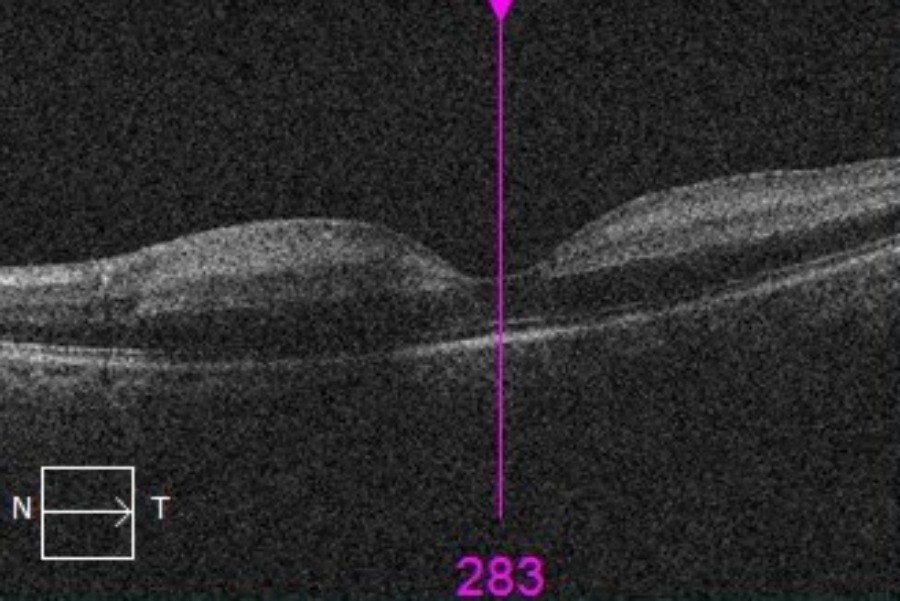
Optical coherence tomography of the left eye demonstrated increased retinal reflectivity and inner retinal thickening (Figure 3). Vital signs were within normal limits. No other focal neurological deficits were noted.


_of_the_left_eye_demonstrating_increased_retinal_reflect.jpeg)
Subcutaneous hyaluronidase was immediately administered with 3000 units (U) to the lower eyelid and 1500U to the peribulbar space. The patient was referred to the Emergency Department (ED) for ongoing management and to rule out a cerebrovascular event. Further dose of 1500U hyaluronidase was injected on arrival to ED. Computerized tomography with angiography of the head and neck was performed which demonstrated no evidence of ophthalmic artery occlusion, acute ischemia or hemorrhagic infarct. The patient was started on 1 g of intravenous methylprednisolone daily for two days. She was then stepped down to 60 mg of oral prednisolone daily.
At subsequent follow up, BCVA remained CF at 1 meter with pinhole improvement to 6/180. Left RAPD was noted. IOP and ocular motility remained normal. The periorbital swelling and ecchymosis had resolved, however, the mild blepharoptosis remained. Anterior segment examination was unremarkable. On fundoscopy, the optic nerve appeared pale with a cup to disc ratio of 0.6. Microaneurysms and exudative changes were noted at the macula. There was no evidence of neovascularization.
Discussion
Cosmetic filler injections are marketed as a relatively safe treatment option for non-surgical facial rejuvenation.6 Of the multitude of side effects and adverse events that can occur, the majority are typically transient and resolve.6 However, severe vascular complications can also occur. A 10-year retrospective study of US Food and Drug Administration (FDA) Manufacturer and User Facility Device Experience (MAUDE) data on aesthetic dermal fillers found that vascular complications accounted for over 10% of the 5,024 reported adverse events related to facial injections.7 Although less common, serious outcomes such as stroke (1.2%), blindness (0.9%), vision impairment (0.8%), and sepsis (0.7%) were also reported.7
The most frequently implicated fillers were Juvederm Voluma XC (HA, 1050 cases), Sculptra (poly-L-lactic acid, 879 cases), and Radiesse (calcium hydroxylapatite, 620 cases).7
Cosmetic injection-related vision loss is a multifactorial process. Intravascular retrograde embolisation from the facial vasculature to the orbital vasculature is currently the most widely accepted proposed mechanism of vascular occlusion leading to vision loss.8,9 Due to the complex vascularity of the face, injection in any region of the face still holds significant risk.10 The anastomotic connections between the external carotid artery (ECA) and internal carotid artery (ICA) systems play a critical role in the pathophysiology of filler-induced vascular occlusion.11 Notably, branches of the ECA such as the infraorbital and angular arteries anastomose with muscular branches and the dorsal nasal artery, which arise from the ophthalmic artery, a branch of the ICA.11 In our patient’s case, it is highly likely that filler material embolized retrogradely through the infraorbital or angular arteries, which then traversed these anastomoses into the ophthalmic artery, which then subsequently proceeded anterograde with the blood flow into the central retinal artery and its distal macular arterioles.11 This accounts for the macular ischemia and vision loss observed and underscores the importance of understanding these vascular connections in preventing and managing filler-related ocular complications. Injection pressure, particle size and expansile properties of the injected filler also contribute to the mechanism, location and severity of the occlusion.9
PDLLA filler, as used in our patient’s case, has become increasingly used in cosmetic procedures given its long-lasting effect and supposed safety profile.5 REGEN Biotech, the manufacturer, reported no serious adverse effects (eg. death, blindness, and skin necrosis) in a study including an estimated 16,000 patients who received PDLLA facial injections from April 2014 to July 2018.12 Adverse effects observed in their study included mild swelling in 50% of patients, 30% reported bruising, and 20% reported pain.12 These adverse effects were largely resolved at subsequent follow up.12 From our literature search, there are four other cases with vision loss secondary to PDLLA injection reported in the literature to date.12–15 To the best of our knowledge, retinal artery occlusion following PDLLA self-injection to the lower eyelid region has not been reported previously.
There have been several proposed treatment strategies in the acute management of cosmetic injection related vision loss. The overarching consensus in the literature is that prompt recognition, diagnosis, urgent commencement of treatment, transfer to an emergency department and early referral to a specialist ophthalmologist is key.16 Treatment options suggested for filler related vaso-occlusion include ocular massage, hyperventilation and nitrates to encourage vasodilation to dislodge the embolus.9,10 Anterior chamber paracentesis and IOP lowering agents have also been used to try to increase blood flow, potentially displacing the embolus and restore perfusion.16 Once in the hospital setting, other treatment options such as hyperbaric oxygen therapy to increase oxygen tension and oxygen delivery to ischaemic retinal tissue; systemic steroids to reduce vascular endothelial oedema; and anticoagulation with agents such as heparin to prevent further thrombosis should be considered. Specifically for HA-fillers, the role of hyaluronidase is included in many published management guidelines, including the guideline published by The Royal Australian and New Zealand College of Ophthalmologists (RANZCO) in 2024.16 In particular, intra- arterial thrombolytic therapy (IATT) with hyaluronidase has been shown to be effective in achieving successful recanalization of the occluded artery with no procedural related complications.17 However, there is a significant lack of treatment options for non-HA based fillers much like in the case of our patient. Although hyaluronidase was administered to our patient, it was unlikely to be of benefit as PDLLA is unable to be broken down by hyaluronidase.18 PLA polymers are biodegradable and bioresorbable, however each have different properties which affect how they can be dissolved.4,19 PDLLA is an atactic and amorphous polymer that has a high solubility in solvents such as benzene, chloroform, dioxane, acetone, toluene, acetonitrile, methanol, and ethyl acetate.4,19 However, although there are solvents that are able to dissolve PDLLA, unfortunately, none of these are safe or approved for injection into the human body.20 These substances are known to be irritants, toxic and harmful if introduced systemically or into human tissues.20 Furthermore, the biostimulatory nature of PDLLA likely results in a more prolonged tissue response, potentially making the acute management of complications more complicated.18 Therefore, the management of complications such as vascular occlusion secondary to PDLLA filler is largely limited to supportive care, not direct chemical dissolution.
Conclusion
We present a further case report of filler blindness caused by PDLLA, a non-HA based filler. Unlike HA based fillers, there is no agent or antidote that can safely dissolve PDLLA should it be required. As the utility and efficacy of current treatment options remain variable and largely limited, with no treatment associated with significant visual recovery, it is important that clinicians understand the properties of the filler used, mechanisms of occlusion, risk reduction strategies and early recognition of these complications. Risks should be carefully considered, with potential complications carefully explained to patients.
Funding
No funding or grant support.
Informed Patient consent
Consent to publish the case report was obtained from the patient in writing. This report does not contain any personal information that could lead to the identification of the patient.