
Introduction
Jejunal diverticula are the least common form of small bowel diverticula, with an incidence of 0.1–1.5% in radiological or autopsy series. They are usually false diverticula, consisting of mucosal and submucosal herniations through the muscular layer, typically at the mesenteric border of the jejunum. While the condition is primarily seen in the elderly due degenerative changes in intestinal smooth muscle or myenteric plexus dysfunction, it is exceptionally rare in young adults. The majority remain asymptomatic throughout life, but a subset can present with complications such as obstruction, hemorrhage, diverticulitis, perforation, or localized abscess formation.
We report a rare case of a 29-year-old male with a single jejunal diverticulum complicated by perforation and interloop abscess formation. The case highlights diagnostic challenges, surgical management, and the importance of considering jejunal diverticula as a cause of acute abdomen even in young adults.
Case Summary
A 29-year-old previously healthy male presented to the emergency department with a 4-day history of lower abdominal pain associated with distension and vomiting. The pain initially began in the periumbilical region and later localized to the lower abdomen. It was constant, moderate to severe in intensity, and aggravated by movement. He reported nausea and anorexia but no diarrhea or constipation. There was no history of abdominal trauma, tuberculosis, peptic ulcer disease, or prior abdominal surgery. He denied alcohol consumption or smoking and had no family history of bowel disease.
On admission, the patient was afebrile, pulse rate 90 bpm, and blood pressure 110/70 mmHg. The abdomen was mildly distended with localized tenderness and guarding in the lower abdomen. No palpable mass was noted, and bowel sounds were sluggish. There were no signs of generalized peritonitis. Digital rectal examination was normal. Initial hematological and biochemical investigations were within normal limit, except the C-reactive protein (CRP) of 66 mg/L. A plain erect abdominal X-ray showed few central air-fluid levels without free gas.
Ultrasound revealed a localized fluid collection with internal echogenic particles between small bowel loops in the left mid-abdomen, suggesting a walled-off abscess. After initial resuscitation and intravenous antibiotics, exploratory laparotomy was planned.
Exploratory laparotomy via a midline incision revealed localized interloop adhesions in the left mid-abdominal region. On gentle separation, approximately 40 mL of thick purulent fluid was drained from a confined abscess cavity between jejunal loops. A single diverticulum measuring about 1 cm in diameter was found arising from the mesenteric border of the proximal jejunum, approximately 90 cm distal to the duodenojejunal flexure. The diverticulum showed a pinpoint perforation at its base, communicating with the abscess cavity. The surrounding jejunal wall appeared inflamed but viable. No additional diverticula were found elsewhere in the small intestine or colon. Segmental resection of about 20 cm of the affected jejunum containing the perforated diverticulum was performed, followed by single-layer end-to-end hand-sewn anastomosis using 3-0 absorbable sutures. The peritoneal cavity was irrigated with warm saline until no further residue, and a drain was placed in the pelvis.

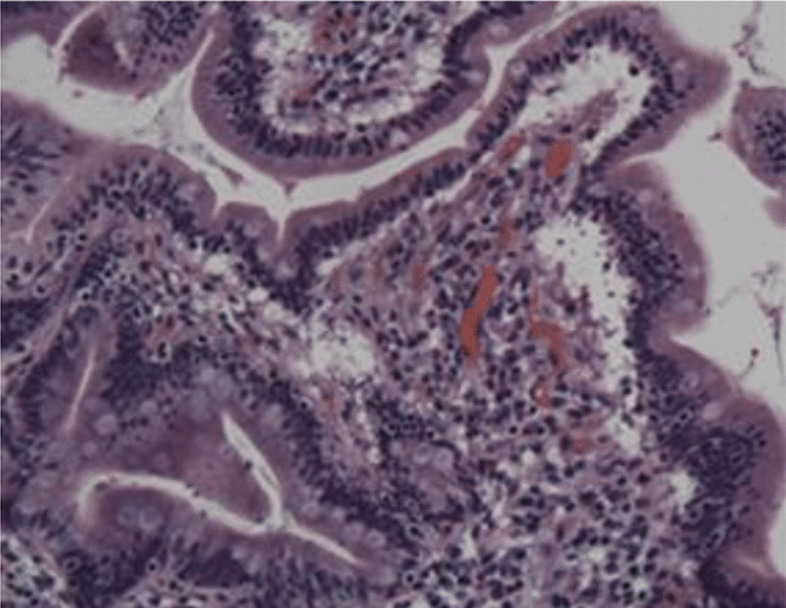
The patient had an uneventful postoperative recovery. Nasogastric tube was removed on postoperative day 2, and oral intake was resumed on day 3. The drain was removed on day 5, and the patient was discharged on day 6 in good condition. Histopathological examination of the resected segment revealed a true diverticulum containing all layers of bowel wall with focal ulceration and acute inflammatory exudate at the perforation site. There was no granulomatous inflammation, dysplasia, or malignancy. At 3-month follow-up, the patient remained asymptomatic with normal bowel habits and weight gain.

Discussion
Jejunal diverticula are rare, accounting for only about 18% of small bowel diverticula, and they predominantly affect older adults. Reports in patients younger than 30 years are extremely rare. The rarity in young individuals suggests that congenital factors or focal wall weakness may play a role when they do occur early.
Jejunal diverticula can be true or false. False diverticula, which are more common, involve only mucosa and submucosa herniating through the muscularis layer at points of vascular entry. True diverticula, though rare, contain all layers of the bowel wall and are sometimes congenital in origin. Increased intraluminal pressure, disordered peristalsis, or localized wall weakness contribute to their development. The diverticulum in our patient was histologically a true diverticulum, possibly congenital.
Most jejunal diverticula are asymptomatic. When symptoms occur, they are often nonspecific — intermittent abdominal pain, bloating, or malabsorption. Acute presentations occur when complications arise; such as – diverticulitis, perforation, hemorrhage, obstruction and abscess formation. Perforation leading to interloop abscess is particularly rare but potentially life-threatening if not recognized promptly. In this case, the contained perforation led to a localized interloop abscess, avoiding diffuse peritonitis and allowing a more localized clinical picture.
Preoperative diagnosis remains challenging due to nonspecific symptoms and low clinical suspicion, particularly in young patients. Imaging plays a key role - Ultrasound may detect localized collections. CT scan is the investigation of choice, demonstrating diverticular outpouchings, bowel wall thickening, and abscesses. We did not procced with CT scan because of deteriorating patient clinical picture.
Differentials in a young adult with localized small bowel abscess include - Meckel’s diverticulitis, Crohn’s disease with penetrating abscess, tuberculous enteritis, perforated jejunal ulcer and foreign-body perforation. Histopathology helped exclude Crohn’s disease and tuberculosis in this case.
The management approach depends on the severity and extent of disease. Uncomplicated diverticulitis is managed conservatively with bowel rest and intravenous antibiotics. Localized abscesses may be treated with image-guided percutaneous drainage in selected patients, whereas perforation or generalized peritonitis warrants prompt surgical intervention. The ideal surgical approach for perforated jejunal diverticulum is segmental resection of the affected segment with primary anastomosis. Simple diverticulectomy is discouraged due to the risk of anastomotic leak and recurrence, especially if surrounding bowel is diseased. In this case, segmental resection with primary anastomosis was curative, and postoperative recovery was smooth.
Histopathological analysis is essential to confirm the diagnosis and exclude other pathologies such as Crohn’s disease, tuberculosis, or neoplasia. Our patient’s specimen confirmed a true diverticulum with acute inflammation and perforation. The long-term prognosis after surgical resection is excellent, with a very low recurrence rate when the diseased segment is completely removed. Nutritional outcomes and bowel function are usually preserved.
Only a few cases of jejunal diverticulitis or perforation have been reported in young adults. Most literature emphasizes its occurrence in older populations, likely secondary to degenerative changes in smooth muscle or myenteric plexus dysfunction.
A review by Kassir et al. (2015) noted that fewer than 5% of reported jejunal diverticulitis cases occurred in patients younger than 40 years. The present case thus represents an unusual early-onset presentation with abscess formation — a clinical rarity.
Conclusions
Jejunal diverticulum is an uncommon cause of acute abdomen, especially in young adults. Perforation leading to an interloop abscess is a rare but serious complication. Early recognition with CT imaging and timely surgical intervention are key to favorable outcomes. Surgeons should consider this rare entity when faced with unexplained localized intra-abdominal abscesses, even in younger patients. Segmental jejunal resection with primary anastomosis remains the treatment of choice, providing excellent outcomes.