Introduction
Gastric pneumatosis is defined as air or gas in the stomach wall.1–3 Normally, the stomach is the least common location for intramural gas in the gastrointestinal tract.4,5 Therefore, gastric pneumatosis is rare. It can be classified into two types: gastric emphysema (GE) and emphysematous gastritis (EG). The causes, symptoms and outcomes are different between these two entities.6 GE is usually asymptomatic and generally secondary to mechanical causes.7,8 EG is secondary to an infection in the gastric wall by the gas-producing organisms.6 GE usually presents with mild symptoms, able to be managed conservatively, self-limiting; and surgery can be avoided. EG, on the other hand, is critical; has a severe prognosis, high probability of complications, and a high mortality rate of 61%1
We report a case of gastric emphysema after two episodes of forceful vomiting of frank blood at Kasemrad Rattanathibed Hospital in Bangkok, Thailand.
Case Presentation
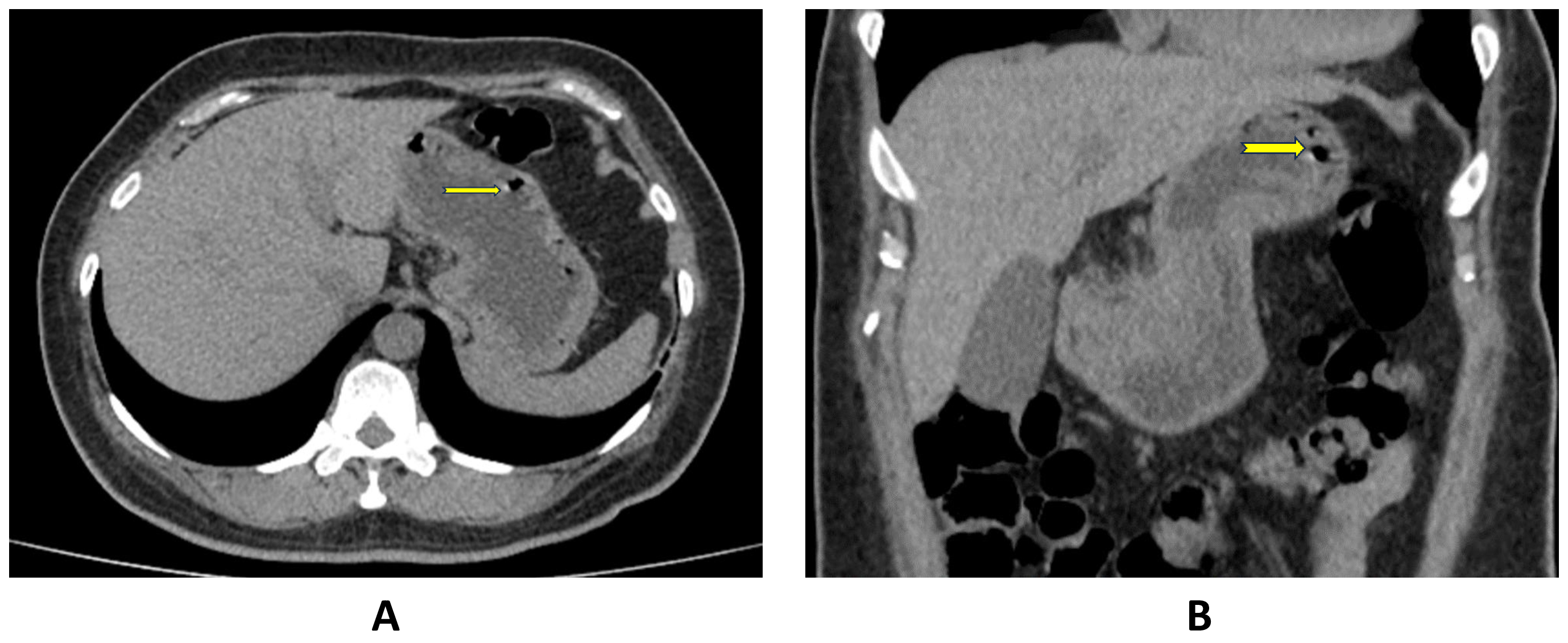
A 52-years-old female patient with underlying hypertension, dyslipidemia and anemia due to alpha thalassemia [hematocrit of 21% (normal range of 37-46%) was on treatment with proton-pump inhibitor for dyspepsia, persisting nausea and vomiting. She presented to our emergency department with vertigo, severe nausea and vomiting. She developed 2 episodes of severe frank-blood vomiting followed by syncope. She was found to have hypotension (BP 100/60 mmHg) and anemia (hematocrit 20%). A gastric lavage showed coffee-ground content. A computerized tomographic (CT) scan of abdomen was performed and showed numerous air bubbles in the wall of stomach at the fundus and along the greater curvature of cardia (Figure 1).
_and_coronal_(b)_ct_scan_images_showing_air_bubbles_in_gastric_wall_at_the_fundus.png)
An urgent esophagogastroduodenoscopy (EGD) was performed and showed an ulceration at the lesser curvature. Biopsies of the ulceration showed no evidence of malignancy.
The patient was started on intravenous proton-pump inhibitors (PPIs) and received blood transfusion (a total of 2 units of packed red blood cells) that increased the hematocrit from 21% to 28%. The remainder of the hospital course was unremarkable, and the patient was discharged to home in a stable condition after 4 days of hospitalization, with oral PPI therapy.
Discussion
Gastric pneumatosis is defined as air in the wall of stomach without any underlying infection,9 It is a relatively rare clinical entity with only 100 cases reported in the literature in the last three decades10 There are two types of gastric pneumatosis: emphysematous gastritis (EG) and gastric emphysema (GE). GE must be differentiated from EG in terms of presentation and management11
EG may occur by inoculation of the gas-producing bacteria into the gastric mucosa or by hematogenous spreading. Clostridium perfringens, Escherichia coli, Pseudomonas aeruginosa, Streptococci, Staphylococci, and Enterobacter species are the most frequent causative agents.12 The affected patients are usually very ill with severe abdominal pain, peritoneal sign, and often in septic shock resulting in a high rate of mortality. Surgery may be required in some critical cases.12–14
This review will focus only on GE. There are numerous major causes of GE include gastric outlet obstruction (secondary to malignancy, structure, volvulus, pyloric or duodenal stenosis), trauma (secondary to endoscopy, nasogastric tube, instrumentation) and/or ischemia.10 Gas from extra-gastric sources can travel to the stomach wall as well; for instance, from small bowel, colon and appendix or even from lung dissecting along the interstitial planes.15 Other causes include air leakage from the alveoli or mediastinum in obstructive lung disorder or pneumothorax; gastric dilatation from eating disorders like bulimia or anorexia nervosa; blunt abdominal trauma; cardiopulmonary resuscitation; connective tissue disorders; diabetic gastroparesis; ingested toxins; pancreatitis; and/or cytotoxicity of chemotherapeutic agents such as Cyclophosphamide, Adriamycin, Vincristine, and high-dose Dexamethasone.2
There are numerous risk factors for GE, including gastric ischemia, aberrant arterial anatomy, atherosclerosis, hypertension, dyslipidemia, weakened gastric wall due to connective tissue disorders, asthma, alcoholism, pancreatitis and diabetes mellitus.2 In the presented case, the cause of GE was severe vomiting.
To date, there are only 14 cases of vomiting-related GE that were reported in the literature.2 Most patients present with nausea, vomiting, and upper abdominal pain. Hematemesis due to gastric mucosa tear is occasionally noted. Intractable vomiting increases gastric pressure and causes trauma or tear of the gastric mucosa, creating an access point for air to infiltrate the gastric wall.16 Vomiting-induced GE involves all age group ranging from 9 months to 81 years.17 Etiologies of vomiting are different in different age groups. In pediatric patients, the most common cause of GE is gastric obstruction by pyloric stenosis. In elderly patients, ischemia, gastric outlet obstruction due to malignancy or stenosis, and trauma are the most common causes.
Clinical manifestations of GE are usually nonspecific with nausea, vomiting, and epigastric or abdominal pain. Most patients are hemodynamically normal without signs of an acute abdomen requiring surgical intervention. In general, the clinical course is usually benign and self-limiting without clinical complications.10,18
The diagnosis of GE can be confused with EG which is fatal, since both conditions have somewhat similar initial clinical presentation and laboratory findings. Although a plain radiography of chest or abdomen is usually adequate for initial detection of GE, a contrast-enhanced CT of the abdomen remains the study of choice in diagnosing GE. Not only it can detect the small amount of gastric wall air that is missed from plain radiography, but also evaluates the entire abdomen to rule out other underlying pathologies2,9,13,15 Ultrasonography is another alternative to CT in some selected patient.9
Abdominal CT scan imaging is also very important in differentiating between GE and EG. GE usually appears as a linear distribution of air without gastric wall thickening while in EG, it appears as a streaky distribution of air with gastric wall thickening.2 However, radiologic findings alone are not sufficient for making a definitive diagnosis. The risk factors, clinical presentation, and other biochemical studies should also be taken into consideration in the differential diagnosis. In some cases, a definitive diagnosis is made only after endoscopy or surgery, such as in patient with gastric ischemia.12
Since most of the GE patients are hemodynamically normal, conservative management including bowel rest, gastric decompression, intravenous fluids, antiemetics, antibiotics, and proton-pump inhibitor is usually sufficient.19,20 Follow up CT scan imaging usually shows resolution of air in 3-4 days. However, if when patients are hemodynamically unstable and with sign of an acute abdomen, immediate surgical exploration is warranted. In inconclusive cases, urgent endoscopy or diagnostic laparoscopy are required.2
Conclusions
Gastric emphysema is a rare condition that can also occur after forceful emesis. While most cases of gastric emphysema are successfully managed non-operatively, maintaining a high index of suspicion for this condition and understanding the diagnostic importance of CT scan imaging of the abdomen, are crucial for avoiding diagnostic delays.