
Introduction
Mesenteric hematomas from traction on incarcerated bowel within inguinal hernias are very rare, with only two cases being reported in the English literature.1,2 We report a case of a hematoma within the mesentery of the sigmoid colon of a patient with a chronically incarcerated left inguinal hernia containing a loop of sigmoid colon.
Case Description
The patient is a 71-year-old male with multiple comorbidities including orthostatic hypotension, cognitive decline, schizoaffective disorder, obesity, and constipation.
He presented to the emergency department with one day of left lower quadrant (LLQ) pain while straining to have a bowel movement. He denied blood in his stool.
On physical examination of the abdomen, the patient reported mild lower abdomen tenderness, without rebound or signs of guarding. A large (20 x 20 cm), non-reducible left inguinal hernia descending into the scrotum was palpated without tenderness or overlying skin changes. The patient was afebrile, normotensive, and with a normal heart rate. His complete blood cell count, chemistry, and coagulation profile were normal, including his lactic acid level.
An initial computed tomography (CT) scan of the abdomen and pelvis without contrast showed a lower intra-abdominal mass (6.1 x 9.2 x 6.1 cm), and a large left inguinal hernia containing fat, segment of urinary bladder, and a loop of sigmoid colon. (Figure 1). To further differentiate between a mesenteric mass and a hematoma, a CT angiogram of the abdomen was obtained that confirmed the diagnosis of a hematoma of the sigmoid mesentery proximal to a herniated loop of sigmoid colon. There was no evidence of active bleeding.
_and_the_left_in.jpg)
Given the lack of reported recent trauma to the abdomen, absence of anti-coagulation medications, normal coagulation profile, and onset of LLQ pain after straining in a patient with an incarcerated left inguinal/scrotal hernia containing a segment of sigmoid colon, we suspected that the proximal sigmoid mesentery hematoma is the result of vascular traction injury from the herniated distal sigmoid colon.
After a shared decision making, the patient was taken to the operating room for an open surgical repair of the left inguinal hernia.
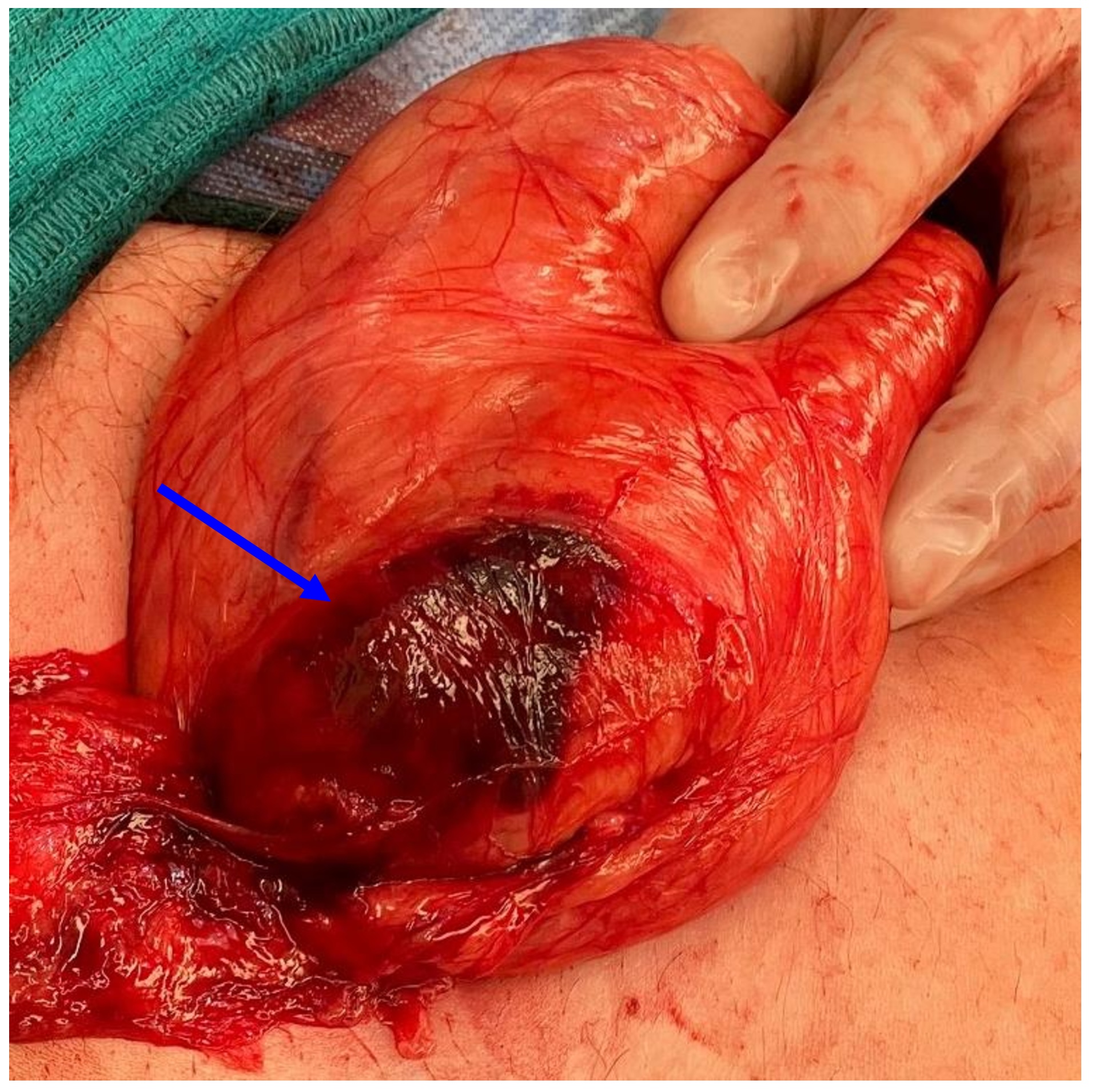
An incision was made in the left groin and the external oblique muscle was opened to reveal the contents of the inguinal canal. After the hernia contents were isolated from the spermatic cord, we opened the sac and used gentle manual traction on the sigmoid colon to externalize the mesenteric hematoma for inspection (Figure 2). The hematoma remained stable after 10 minutes of observation. We then fully reduced the sigmoid colon and its mesentery into the abdomen and closed the peritoneal sac, before repairing the hernia with mesh. The patient’s post-operative course was uneventful, and he was discharged home on postoperative day 2. He was seen in the clinic for regularly scheduled follow up and was without complications at that time.
_of_the_sigmoid_colon_mesentery.jpg)
Discussion
Mesenteric hematomas are a rare clinical condition that occur spontaneously or as the result of abdominal trauma or an iatrogenic event.3 The occurrence of a spontaneous mesenteric hematoma has been well described in literature due to anticoagulant use, collagen disorders, vasculitides, or aneurysms4,5 Spontaneous mesenteric hematoma has also been described in the literature as being idiopathic. In approximately 40% of reported cases of mesenteric hematoma, the source of bleeding is never found.6 Our report expands upon the known causes of spontaneous mesenteric hematoma formation by detailing a case study of a traction-related mesenteric hematoma of the sigmoid colon in conjunction with a chronically incarcerated left inguinal hernia.
This report adds to only two other cases of traction-induced spontaneous mesenteric hematomas currently described in the literature. First, Sutton et al,1 described the case of a 67-year-old male who presented with increasing abdominal pain caused by the recurrence of a right inguinal hernia, that was found to have pulled upon the mesenteric vasculature as it became incarcerated, forming a spontaneous traction-induced hematoma of the mesentery within the hernia sac. Hahn et al,2 later described an 89-year-old male with a spontaneous stable mesenteric hematoma caused by a herniation of the sigmoid colon that produced a traction injury on the mesenteric vasculature.
The management of mesenteric hematoma depends on the clinical presentation. Reported cases of mesenteric hematoma display physical symptoms including abdominal distension, pain, or tenderness, palpable abdominal masses, and nausea.7–9 The nonspecific physical symptoms of mesenteric hematomas make it difficult to diagnose based on physical examination alone. Most reported cases required imaging studies to identify the mass which include contrast enhanced CT scans, ultrasound, and magnetic resonance imaging.1–10 In multiple cases, the results of the CT scans are nonspecific and require further imaging studies to differentiate between a mesenteric mass, gastrointestinal stromal tumor, or a mesenteric hematoma.10 When pseudoaneurysm or arterial-aneurysm is suspected, an angiography or gallium (GA)-scintigraphy may be performed to identify the source of bleeding.4 When CT scans are inconclusive and the patient displays signs of active bleeding, emergent laparotomy has been performed to diagnose and identify the source of the mesenteric hematoma.6,8 In our case, a CT angiogram of the abdomen confirmed the diagnosis of a hematoma of the sigmoid mesentery proximal to the herniated loop of sigmoid colon, with no evidence of active bleeding.
Conservative management has been shown to be successful in treating small or medium-sized, stable mesenteric hematomas, often through correction of coagulation abnormalities and close patient monitoring.11 Conservative management may include fluid resuscitation, interval imaging studies, and regular follow-up appointments.12 Fluid resuscitation serves to replenish fluids lost due to bleeding, and interval imaging studies allow for the clinician to monitor for the resolution of the hematoma. In unstable cases, transcatheter angioembolization has been utilized as a minimally invasive procedure to treat the bleeding in the mesenteric vasculature. Phua et al11 described the use of angioembolization to treat active mesenteric bleeding in a patient deemed high risk for emergent laparotomy.
Surgery is indicated if the patient shows signs of severe blood loss or secondary complications such as intestinal obstruction or ischemia.3 The most common surgical intervention to treat mesenteric hematomas is a laparotomy coupled with hematoma evacuation.2,4 Resection of affected bowel may be indicated in the case of active bleeding, bowel obstruction, or frankly ischemic bowel.5,6 Mesenteric hematomas caused by vascular traction due to inguinal hernias may be evacuated at the time of hernia repair.2 However, similar to our report, Sutton et al1 repaired the hernia, but chose not to intervene on the hematoma, electing for the hematoma to resolve on its own. As postoperative bleeding complications are possible after inguinal hernia repairs, the close maintenance of hemostasis during the operation is of critical importance. In the presence of a large mesenteric hematoma, especially those encompassed within an incarcerated hernia sac, extreme care must be taken. Surgical manipulation of a large hematoma can result in significant intraoperative complications as well, such as rapid cardiac decompensation and loss of vascular tone.11
Conclusions
Mesenteric hematomas due to traction injury are a very rare occurrence, with our patient being only the third reported case in the English literature. Despite the rarity of this diagnosis, spontaneous mesenteric hematomas should be considered in the differential diagnosis for mesenteric masses coinciding with incarcerated inguinal hernias on imaging studies. Our report highlights the importance of timely repair of inguinal hernias, as bowel incarceration into the hernia sac could lead to traction injury of the mesenteric vasculature.