

Introduction
A pseudomeningocele (PM) represents an abnormal collection of cerebrospinal fluid in the perispinal space that communicates with the arachnoid space via a dural fistulous track.1–4 Pseudomeningocele was first reported by Hyndman and Gerber2 in 1946. Iatrogenic PM is an uncommon with an incidence (5-18%) and challenging complication most commonly caused by lumbar surgery such as diskectomy.5–8 Despite its rarity, iatrogenic PM is associated with increased medical costs and high morbidity and mortality.5–7
In this article, we report on a patient that underwent a micro-discectomy for a left lumbar disc herniation (L5-S1), followed by a re-do microdiscectomy due to a re-herniation. Unfortunately, his second surgery was complicated by a cerebrospinal fluid leak leading a PM. Over time, this PM grew despite conservative measures. The PM resolved after percutaneous injection of a fibrin sealant into the dural fistula tract.
Case Description
Our patient is a 51-year-old male who presented with lower back pain and left leg pain radiating to the posterior thigh and to the foot. MRI showed a large left subarticular disc extrusion at L5-S1 resulting in moderate to severe thecal sac narrowing, as well as severe left
subarticular zone narrowing and mass effect upon the left S1 nerve root. He denied any weakness or numbness, as well as saddle anesthesia or bowel or bladder incontinence. His pain level was 3/10 with walking and worsened with sitting to 5/10. He was first treated conservatively with pain control measures and physical therapy, but his symptoms were refractory to conservative management.
After failing conservative therapy, he underwent a L5-S1 laminectomy and left microdiscectomy for the left L5-S1 disk herniation that was the cause of his symptoms.
Following the surgery, the patient did very well with complete resolution of the symptoms for 1 year until he unfortunately developed recurrent symptoms of radicular leg pain down the left leg reminiscent of his original pain. This was significantly limiting his activities of daily living and repeat imaging was performed that demonstrated a recurrent disc herniation at this level causing compression of the nerve root and correlating with his symptoms.
MRI showed a left subarticular disc extrusion at L5-S1 that resulted in compression of the left S1 nerve root. The left S1 nerve root distal to the compression was asymmetrically enlarged with increased T2 signal that may reflect inflammation and edema. There was also mass effect on the left S2 nerve root at this level. Additionally, there was a thin transversely oriented curvilinear T2 hyperintense focus along the dorsal aspect of the cauda equina nerve roots at the L3-L4 through L4-L5 levels, with prominence of dorsal cerebrospinal fluid (CSF) intensity in this region. This is nonspecific and could reflect intrathecal scar/adhesion, possibly a small arachnoid cyst, or chronic subdural collection. Finally, there was a CSF intensity fluid collection in the L5 laminectomy surgical bed. This finding is nonspecific and could represent a postoperative seroma, though the possibility of a pseudomeningocele could not be excluded at that time.
The patient underwent a redo left L5-S1 microdiscectomy for the recurrent disc herniation, which again worked well in terms of the patient’s pain. His pain was largely resolved from removing the herniating disc and thereby taking pressure of the affected nerve roots.
A post-operative MRI (Fig. 1) demonstrated extradural CSF intensity in the left aspect of the spinal canal and pockets of CSF intensities in the posterior paraspinal muscles and in the overlying soft tissues consistent with CSF leak/pseudomeningoceles. Of note, there was a possible dural discontinuity along the left aspect of the thecal sac at the level of L5-S1, where surgeries were conducted.
__axial_t2_(b)__and_axial_3d_t2_cube_(c)_images_of_the_lumbar_spine__demons.png)
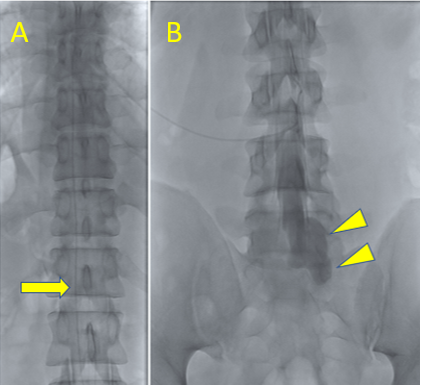
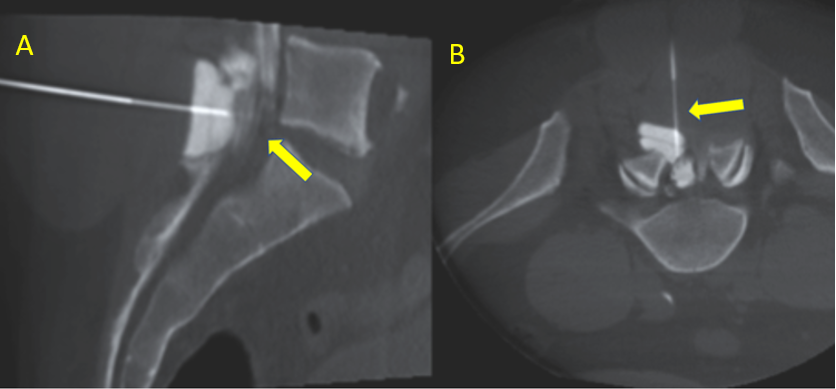
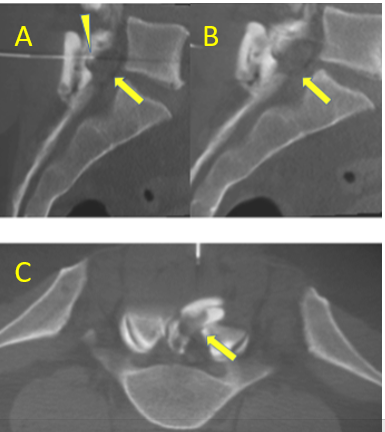
To prevent another surgery to attempt to repair the CSF leak, we opted to conduct an image-guided, percutaneous closure of the PM by injection of fibrin sealant in the fistulous tract of the PM close to the spinal canal. After prepping and draping the back of the patient in prone position in a sterile manner, a lumbar drain was placed for reduction of intraspinal CSF pressure and myelogram (Fig. 2). Under fluoroscopic cone-beam guidance, a 19 G introducer needle was then advanced into the posterior peri-lumbar fluid collection (Fig. 3). A 20 G x 15 cm needle was then placed through the 19 G introducer needle close to the neck of the pseudomeningocele (Fig. 3), and through the 20 G needle, approximately 7.5 ml of DuraSeal dural sealant (1.5 vials) injected into the neck of the pseudomeningocele adjacent to the lower 5th lumbar spinal sack (Fig. 4). Post-sealant placement, cone-beam study showed successful placement of the dural sealant. Then, approximately 100 cc of clear spinal fluid was aspirated from the perilumbar collection via the 19 G introducer needle to decompress the pseudomeningocele. Post-procedure cone-beam study demonstrated significant interval decrease in size of fluid collection. The patient tolerated the procedure well without any immediate post-procedure complications and returned to floor in stable condition. The lumbar drain was kept in for 3 days for CSF diversion and then was removed without any issues.
_showing_lumbar_drain_(arrow)_(b)_myelogram_in_frontal_view_of_lumbar_myelogram_demonst.png)
_under_cone-beam_ct_guidance_in_a_sagittal_view_(a)_and_a.png)
_and_completion_(b)_of_the_fibrin_deposition_via_the_needle_(arrowhead)_demonstr.png)
For a few weeks after the procedure, he developed intermittent headache, neck stiffness and fever, which prompted presentation to medical attention. Workup including ESR, CRP, WBC and microbiology culture returned negative for a bacterial meningitis. The symptoms also resolved with minimal pain control medication. Therefore, he was determined to have an aseptic meningitis, likely from fibrin glue breakdown. He was further managed symptomatically with a steroid trial.
On his last follow up visit, he reports feeling great. The symptoms of aseptic meningitis have completely resolved. He has returned to all his usual activities, including ADLs and hobbies including running. The CSF leak has resolved given his completely flat back without any palpable swelling or fluid collection as shown on the follow-up MRI (Fig. 5). His radicular pain is also completely gone.
_and_6_months_post-percutaneous_repair_(b_d)_mr_images_.png)
Discussion
Laminectomy and microdiscectomies for herniated lumbar discs are among the most common neurosurgical procedures.3–6 These are highly safe procedures routinely conducted throughout the world at many different types of hospitals ranging from major academic centers to outpatient day surgery practices. Complications associated with laminectomy include infection (< 1%), dural tear and spinal fluid leak, reherniation/recurrence of the symptoms needing reoperation, nerve injury causing neurologic symptoms, and persistent pain.3–8
Iatrogenic CSF leak or PM is a known complication after laminectomy, with an incidence ranging from 1-18 % after laminectomy.3–8 CSF leakage can be reduced by the placement of a lumbar drain for CSF diversion and reduction of intraspinal pressure. Prevention of CSF leakage is important for facilitating wound healing, for avoiding positional headaches and for preventing herniation of neural elements through the dural defect, which may cause pain syndromes or neurological deficits. It is generally accepted that reduction of intraspinal CSF pressure often with a lumbar drain facilitates healing of a dural defect in conjunction with maintenance of strict bed rest.3–8 .
Application of fibrin glue sealants (FGS) has been widely accepted as a treatment for CSF leakage.9,10 The FGS can be prepared autologously in the operating room, from cryoprecipitate obtained from the blood bank, or from commercial kits made from donated blood products. Regardless of the origin, fibrin glue sealants, when applied in the dural repair, dramatically increase the rate of healing. The use of dural replacements is more controversial. Repair with fascia, AlloDerm, DuraGen, or other techniques is more a matter of choice than evidence-based medicine.6–8
Primary repair of a dural violation, when possible, is clearly indicated. Multiple surgeons have documented increased infection rates and decreased fusion rates when surgery is associated with CSF leaks.6–8 In addition to CSF leaking from the durotomy, nerve roots have been known to herniate into the durotomy and result in painful syndromes.
A tight, multilayer closure is critical to prevent local CSF collections from leaking outward to the skin. If a CSF leak exists, organisms have a portal of entry and may cause meningitis.6–8 Any CSF leak should be treated immediately by oversewing of the wound and institution of some form of CSF pressure–reducing strategy. The decision to revise a wound rather than treat conservatively depends on several factors, including the tightness of the dural and fascial closure, the presence of and size of the subfascial collection, and the patient’s underlying ability to heal a wound spontaneously.6–8 A CSF pseudomeningocele, even in the absence of an external leak, can increase the likelihood of local infection.6–8
Most CSF leakage cases will close without surgical or interventional management. A direct primary repair of durotomies identified intraoperatively at the time of the leak is the best method for preventing CSF leak after a durotomy.3–8 However, this can fail to prevent a CSF leak in ~5.5% of cases.10 In these cases, or in cases where an occult CSF leak has occurred without an obvious durotomy intraoperatively, temporary CSF diversion via a lumbar subarachnoid catheter can allow a dural defect to heal in 90 % of cases.11–13 Some authors have also reported success with an epidural blood patch although to our knowledge no known large study has assessed the success and complications of this approach. For the patients with whom CSF diversion and primary dural closure at the time of the procedure has failed, our approach may represent a means to heal the defect without the need for a further operation.8–13
PM typically presents within the first 1-2 postoperative/postprocedural months and is suspected in patients with persistent and/or large CSF leaks.3–10 Clinical symptoms, though nonspecific, include fluid collection under the skin, occasionally causing leakage through the skin if the skin is not intact or there is too much pressure from the accumulating PM. Workup begins with CT scan or MRI, which will demonstrate a persistent or increased CSF leak and PM.12 These imaging studies may help to identify the exact location of the fistula, in addition to demonstrating extension of the PM. MRI findings associated with PM include a fistulous track, extradural fluid collection, and PM.12
By describing the successful treatment of a PM with percutaneous injection of a fibrin sealant into the fistula tract of PM we hope that our report contributes to the PM treatment literature as only a few cases of percutaneous PM treatment with fibrin sealant have been described.9,13 Retrospective studies noted success with this method.12 In gigantic leaks, as in this case, it needs myelographic guidance to precisely direct the percutaneous needle to the fistulous entry site for effective deposit of the fibrin. With this technique, only a small amount of fibrin is needed. We also placed a lumbar drain prior to the fibrin injection, which was kept in place for several days to divert the fluid from the fistulous site and reduce the CSF pressure to ensure and promote the closure of the fistulous connection. This technique, using myelographic guidance to direct the fibrin deposit close to the neck of the dural fistula, has not been previously described.
Conclusion
Pseudo-meningocele represents a significant challenge requiring a multidisciplinary approach. Currently, the primary management of pseudo-meningocele is conservative, with further interventions determined based on patient factors and response to initial therapy. While large-scale studies of percutaneous fibrin dural sealant are needed to determine the long-term efficacy of these options, they pose a less invasive option for patients who failed other options, are not operative candidates, or wish to avoid the morbidity of a major operation.
Correspondence Author
Ducksoo Kim, MD, FSIR
Boston University School of Medicine
Department of Radiology
Boston VA Health Care
1400 VFW Parkway, West Roxbury, MA, 02132, USA
Tel: +1-857-203-6414
Fax: +1-857-203-5738
Disclosure Statement
The authors have no conflicts of interest or financial disclosures to declare.