Introduction
Perforated peptic ulcer is a surgical emergency associated with high rates of mortality and morbidity. Surgery remains the standard of care in the management of perforated peptic ulcers in the presence of hemodynamic changes.
We report a case of simultaneous presentation of a contained perforated duodenal ulcer with Lyme carditis causing hemodynamic changes that influenced surgical decision making.
Case Description
A 77-year-old male patient with multiple comorbidities that included chronic kidney disease, cerebral-vascular accident, remote cholecystectomy, hypertension, progressive cognitive decline, failure to thrive and hypotension episodes over the last year, alcoholic abuse disorder with active drinking, and peptic ulcer disease presented to our emergency department with nausea, mild epigastric pain, and poor oral intake.
On physical examination of the abdomen patient had mild tenderness in the epigastrium. On presentation he was afebrile, but intermittently hypotensive (86/45 mm Hg) and bradycardic (50 beats/min). His blood urea nitrogen was 64 mg/dL (normal range 7 – 25) and creatinine was 3.2 mg/dL (normal range 0.5 – 1.5) which were consistent with his known chronic kidney disease. The remainder of chemistry, blood cell counts, liver function tests, lactic acid level, and coagulation tests were all normal. EKG showed sinus bradycardia (55 beats/min) and first-degree atrioventricular (AV) block that were present in the past.
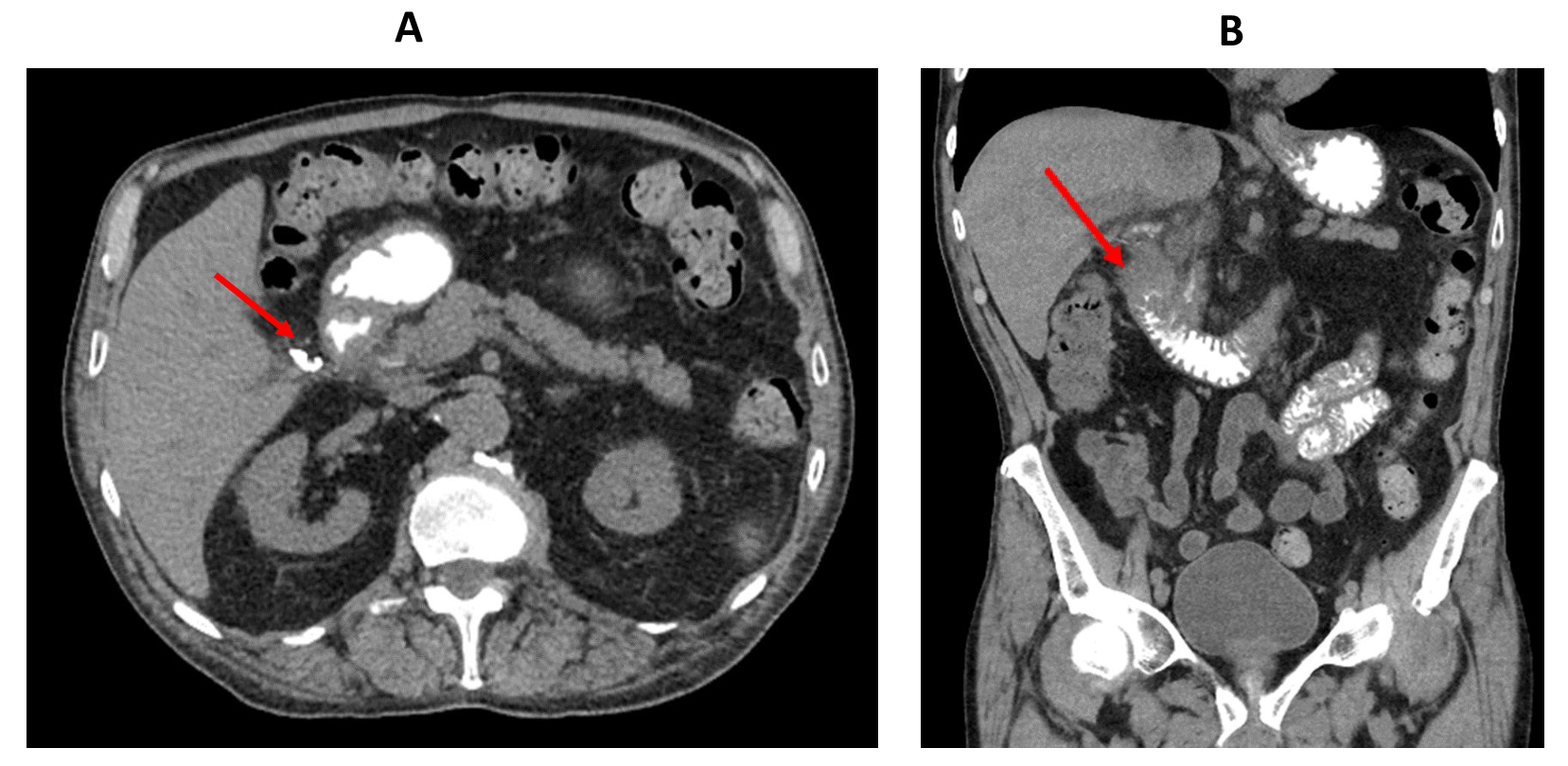
A computed tomography (CT) scan of the abdomen with intravenous and oral contrast obtained in the emergency department showed segmental wall thickening of the second part of the duodenum and duodenal bulb with adjacent fat stranding. There was also a pocket of gas in the medial aspect of the duodenum which was filled by extravasated oral contrast suggesting a contained duodenal ulcer perforation. (Figure 1).
_axial_ct_scan_of_the_abdomen_showing_extravasated_oral_contrast_outside_the_duodenum_(.png)
After the risk and benefits of surgical versus non-operative management of a likely contained perforated duodenal ulcer patient agreed with surgery given presence of hypotension. As such, after intravenous fluid resuscitation was started and broad-spectrum intravenous antibiotics (Ceftriaxone + Flagyl) and intravenous proton pump inhibitors (Protonix) were administered, patient was taken to the operating room for an emergent laparotomy. Exploration of the abdomen revealed no intra-peritoneal evidence of gastric or enteric succus to suggest an active duodenal perforation. After we fully mobilized the first three portions of the duodenum we identified a very inflamed and thickened duodenal bulb that was adhered to the gallbladder fossa.
Next, we performed three air-tests of the duodenum by insufflating air into the stomach via a nasogastric tube while manually and sequentially compressing the second and the third portion of the duodenum, while the duodenum was immersed under warm saline irrigation. The tests did not reveal any air bubbles.
The duodenal bulb remained fused to the gallbladder fossa. Because the pre-operative CT scan suggested the oral extravasation in this area, we were very careful not to lyse these adhesions since we considered it to be very likely that the duodenal perforation could be contained by these adhesions. Despite the lack of an active perforation, we created two vascularized omental flaps. One flap was placed over the second and third portions of the duodenum. The second flap was placed over the adhesion block constituted by duodenal bulb/pylorus/gallbladder fossa. To maintain this flap in place, we sutured it into the anterior wall of the antrum near the greater curvature using a 2-0 Silk suture. A closed suction drain was then placed with its tip near the duodenal bulb area.
Patient’s post-operative course was marked by sudden intermittent episodes of profound bradycardia (as low as 35 beats/min) and hypotension. An extended work-up was initiated to identify the causes of patient’s hemodynamic changes. Possible causes considered for the hypotensive episodes included hypovolemia, gastrointestinal bleeding, distributive shock, autonomic/neurogenic dysfunction, and bradycardia.
Blood and urine cultures were negative, blood cell counts remained normal, cortisol levels were within normal limits, and Helicobacter Pylori testing was negative. The EKGs showed first-degree AV block with intermittent Mobitz type I (Wenckebach). The Cardiology Team recommended placement of a pacemaker that was declined by the patient as it was not considered within his goals of care. His bradycardia/hypotension episodes were treated with bolus of glycopyrrolate or atropine.
A repeat CT scan of the abdomen with oral contrast on postoperative day 5 showed no evidence of contrast extravasation. The NG tube and the drain were removed, and an oral diet was initiated and tolerated.
Lyme disease serology tests were obtained and were positive. Upon discussing these findings with the patient and his family members, they shared that patient was diagnosed with the Lyme disease 4 years prior. Lyme disease is known to cause carditis and AV block, and it would explain the patient’s history of episodic symptomatic bradycardia that also occurred after he presented to our emergency room with radiographic evidence of a duodenal perforation.
Patient received antibiotic therapy for his Lyme diagnosis. However, he continued to decline the placement of a pacemaker. After continued discussions with our Palliative Care Team, patient decided to transition to hospice care and passed away on post-operative day 82.
Discussion
Lyme disease is the most commonly reported vector-borne disease in the United States with more than 185,000 cases reported from 2015 to 2019. Notably, the growing financial burden of monitoring Lyme disease cases has led health departments in high incidence states to significantly decrease reported cases; recorded cases in Massachusetts decreased from 2933 in 2015 to only 7 in 2019.1 The Northeast and upper Midwest are the 2 primary endemic areas in North America, accounting for more than 90% of reported US cases of Lyme disease.1
Lyme carditis occurs in 1-5% of patients, most commonly manifesting as AV conduction block, ranging from first-degree to complete heart block.2 Patients may present with bradycardia, hypotension, lightheadedness, palpitations, shortness of breath and/or chest pain. Diagnosis of Lyme carditis is based on largely non-specific findings, including ECG demonstrating degrees of heart block, chest radiograph, echocardiogram, magnetic resonance imaging, and rarely endomyocardial biopsy, in conjunction with positive serology for Lyme disease.3 Antibiotics are considered standard treatment with amoxicillin or doxycycline given for mild to moderate cardiac disease and ceftriaxone for severe disease. Although most cases resolve within 1-2 days, heart block can fluctuate and worsen rapidly in rare instances of severe Lyme carditis.
The clinical diagnosis can become further complicated in a perioperative setting. Our patient presented with a perforated duodenal ulcer for which non-operative management was initially considered; however, his clinical course was complicated by hypotension necessitating surgery. In approximately 40-50% of cases, the perforation heals spontaneously through omental coverage or by fusion of the duodenum to the underside of the liver.4 Selection criteria for non-operative management are not clearly defined, but risk factors for failed management include high volume pneumoperitoneum, tenderness on digital rectal exam, abdominal tympany, signs of peritoneal irritation, age over 59, and hemodynamic instability.5 Conversely, advanced age and multiple comorbidities may also make patients poor surgical candidates, potentially making them better suited candidates for non-operative management.
Nonetheless, surgery remains the standard of care for perforated duodenal ulcer. Various surgical techniques include simple suture closure of perforation margins without omentoplasty, with free omental patch (Graham technique), or with pedunculated omental patch (Cellan-Jones technique).5 Antibiotic regimen with coverage of Enterobacter and anaerobic bacteria should be initiated as soon as diagnosis is confirmed.
Our patient was initially diagnosed and surgically treated for a perforated duodenal ulcer complicated by intermittent, cyclic hypotension and bradycardia secondary to Lyme carditis. It is uncertain whether an earlier diagnosis of Lyme disease as a potential etiology for the patient’s hypotension would have changed emergent surgical management, but it could have guided antibiotic choice and post-operative care. Although Lyme disease is not a common cause for hemodynamic instability in the surgical patient, it is important to consider it as a differential diagnosis when practicing in Lyme disease-endemic regions and when more frequent causes of hypotension/bradycardia have been ruled out. Early identification and proper treatment with antibiotics are crucial to lowering the risk of cardiovascular complications, avoiding sequelae, and shortening the duration of the disease, especially important in the perioperative setting.
Conclusions
To our knowledge, we describe the first reported case of Lyme carditis complicating the presentation of a perforated duodenal ulcer. Despite such a rare occurrence, when managing perorated duodenal ulcers surgeons should be aware of the risk of Lyme carditis in patients presenting with hemodynamic instability, especially those with a history of outdoor exposure in Lyme endemic areas.
Correspondence Author
Gentian Kristo, MD, MPH, FACS
Department of Surgery
Veterans Affairs Boston Healthcare System (112-C)
1400 VFW Parkway, West Roxbury, MA, 02132, USA
Tel: +1-857-2013-6966
Fax: +1-857-203-5738
E-mail: gentian.kristo@va.gov
Disclosure Statement
The authors have no conflicts of interest or financial disclosures to declare.