
Introduction
The spinal cord
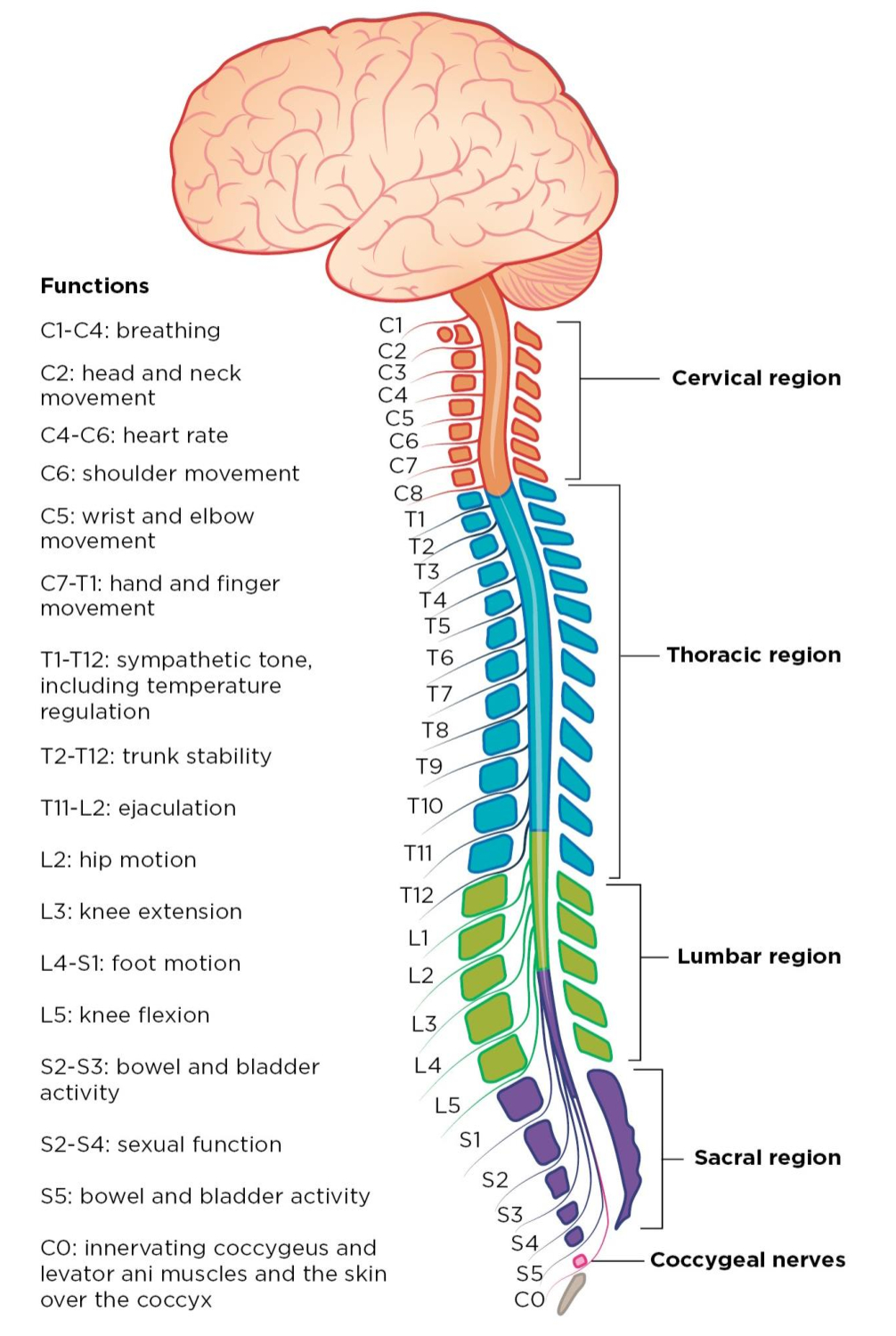
The spinal cord is a long column-like band of nerve tissue running from the base of the skull down to the lower back. It functions as the conduit between the brain and the remainder of the body and conducts both motor and sensory information. The blood supply is primarily from the anterior spinal artery and two posterior spinal arteries. The spinal cord can be divided into four main regions, namely the cervical, thoracic, lumbar, and sacral levels. These levels correspond to levels of innervation throughout the body.1 (Figure 1)
.png)
Spinal cord injuries
The annual incidence of spinal cord injuries (SCI) in the United States alone is estimated to be about 17,000, with the leading cause of SCI being motor vehicle collisions. Other causes include falls, trauma, and gunshot wounds. Injuries can be classified as either primary or secondary. Primary injuries result from direct damage to the spinal cord, such as trauma directly impacting the cord, vertebral fractures, malignancies, hematomas, or abscesses. Secondary injuries are the changes that occur after the initial injury and include pathologies such as inflammation, edema, free-radical formation, tissue damage, and vascular damage.2
Autonomic dysfunction in SCI patients
Autonomic Dysreflexia (AD) is a syndrome characterized by a profound disordered autonomic response to visceral or cutaneous stimuli below the level of spinal cord lesion.3 Clinical manifestations include a sudden increase in blood pressure of at least 20 mmHg from baseline, baroreflex-mediated bradycardia, headache, flushing, sweating, chills, nasal congestion, piloerection, and pallor. Severe hypertension can lead to raised intracranial pressure resulting in seizures, intracranial hemorrhage, myocardial ischemia, arrhythmias, pulmonary edema, and even death.4
Development of AD is influenced by the duration and the level of the spinal injury. Although AD may develop any time following spinal cord injuries, it usually occurs in chronic SCI patients. The incidence of AD is between 50% and 70% in patients with lesions above T65 and increases in frequency with higher level lesions and complete lesions.6 The higher the level of spinal cord injury, the more severe the autonomic dysreflexia symptoms.3,4
The pathophysiology of AD is thought to be a result of a disorganized sympathetic response to stimuli below the level of the lesion7 (Figure 2). The loss of supraspinal inhibitory modulation of spinal sympathetic neurons facilitates a massive discharge of sympathetic preganglionic neurons below the level of the lesion, which can give rise to a profound sympathetic response up to the level of injury, with alterations in vasomotor, pilomotor, and sudomotor activities.3
.png)
When spinal cord injuries are above the T6 level, the splanchnic innervation is activated, causing splanchnic vasoconstriction, and resulting in more severe symptoms such as hypertension and compensatory bradycardia. In patients with SCI below the T6 spinal level, supraspinal sympathetic innervation of the splanchnic vasculature is usually preserved; as a result, autonomic dysreflexia rarely occurs.4
AD is typically triggered by noxious pelvic visceral stimulation, with the most common (approximately 80%) cause being bladder distension.5 Other triggers include acute abdominal pathology, bowel distension, urinary tract infections, skeletal fractures, pressure ulcers, activation of pain fibers, sexual activity, uterine contractions, and even gentle skin stroking.5,8–10
Anesthetic considerations in SCI patients
Pre-operative assessment
As with all patients planned to undergo a procedure requiring anesthesia, the first and perhaps most important step is the pre-operative assessment. In general, a pre-operative assessment includes reviewing the type of surgery, the patient’s medical and surgical history, medications, allergies, and lab work. For SCI patients in particular, these details are exceptionally important. In addition to the medical and surgical history, specifics regarding the SCI are important and outlined as below:
-
Level of injury – for injuries at the cervical spine level, neck range of motion may be limited, affecting intubation efforts
-
Time since injury – succinylcholine, a common paralyzing agent used during induction, can increase the risk of hyperkalemia anywhere from 3 days to 9 months following an injury
-
Sensory level in relation to surgical field – for minor procedures occurring below the level of injury, if sensation is absent, anesthesia may not be needed at all
After verifying the full history regarding the SCI along with the remainder of the medical history, it is vital to pay close attention to certain aspects of the physical exam. The airway assessment is used to predict potential complications intra-operatively, generally with intubation, ventilation, or oxygenation. The exam includes examining dental status, mouth opening, the degree to which the oropharynx can be visualized (Mallampati score),10 thyromental distance and neck mobility.11 For SCI patients in particular, neck mobility may be greatly limited. Other important aspects of the physical exam include assessment of respiratory and cardiovascular status, particularly to understand the patient’s baseline vital capacity, blood pressure and heart rate.12
Access and monitors
Once the patient arrives in the operating room (OR), they will be connected to the standard anesthesia monitors – temperature probe, electrocardiogram, pulse oximetry, blood pressure cuff, and capnography. It is important to obtain a baseline set of vitals prior to any intervention. As with all patients, a suction device, ventilator and anesthesia machine, oxygen, and emergency medications (such as atropine and epinephrine) must all be readily available and functional and pre-oxygenation must be performed. As SCI patients can present with unexpected hemodynamic instability, it is imperative that adequate intravenous access is obtained, either in the form of large bore IVs or central venous catheters. An arterial line will also be helpful for real time blood pressure monitoring.13
Induction and intubation
There is a variety of induction drugs available at the arsenal of the anesthesiologist. The most commonly used medications for induction are propofol, ketamine and etomidate, and they are often administered in conjunction with adjuvants including lidocaine and opioids. Currently, there is no literature to support specific induction drug recommendations for SCI patients. However, it is important to note that patients with SCI often have lower blood volume and reduced muscle mass due to deconditioning, resulting in a smaller volume of distribution for IV anesthetics. Thus, they may react with increased sensitivity to IV induction agents and given the reduction of sympathetic activity to these myocardial depressant agents, these effects may present with dramatic drops in blood pressure. SCI patients also are at a higher risk of renal dysfunction and many of these induction agents are cleared renally. Given these risks, it is reasonable to assume that less-than-standard amounts of these agents are needed to provide adequate induction in SCI patients.14
Neuromuscular blocking agents are administered prior to inserting an endotracheal tube (ETT). As mentioned earlier, succinylcholine is contraindicated between 3 days and 9 months of SCI due to risk of life-threatening hyperkalemia that can result. Non-depolarizing agents such as rocuronium or vecuronium can be safely administered although the mechanism of action is slower, so this must be taken into consideration in emergent cases.
Airway considerations are incredibly important at this point. If a patient has a high-level lesion, usually cervical or high thoracic, or an unstable vertebral fracture, manual in-line stabilization or an awake fiberoptic approach might be necessary for adequate airway access. Minimizing neck movement is crucial for preventing further injury, especially in patients presenting with an acute SCI. Other options include video laryngoscopy and laryngeal mask airways (LMAs), although depending on the type of surgery being performed, an LMA may not be an appropriate choice (i.e., laparoscopic surgery).15
Laryngoscopy and intubation can result in a variety of hemodynamic responses in SCI patients, depending on the level of injury. One study looked at three groups of SCI patients: injury above C7 (quadriplegic), between T1 and T4 (high paraplegic), and below T5 (low paraplegic), along with a control group with no SCI. During intubation, the control group experienced an increase in systolic pressure, heart rate, and plasma norepinephrine concentration. In comparison, the quadriplegic group experienced no change in systolic pressure, a similar increase in heart rate, and minimal increase in norepinephrine, indicating a dampening of the pressor response in this subset. The high paraplegic group experienced an increase in systolic pressure, a marked increase in heart rate and similar increase in norepinephrine, indicating an augmented tachycardic response in this subset. Finally, the low paraplegic group experienced similar effects as the control group in heart rate and systolic pressure rise and had a marked increase in norepinephrine, indicating an exaggerated catecholamine response. It is unclear why the heart rate and catecholamine responses did not correlate within these subsets but nevertheless, it is clear that SCI patients will have varied responses during intubation that the anesthesiologist must be aware of.16
Intraoperative care and complications
If general anesthesia is being performed, either total intravenous anesthesia (TIVA) or inhalation anesthesia are implemented. Both are safe options for SCI patients with no current literature supporting the use of one over the other in this specific population.
The peri-operative time period is crucial for monitoring for vital sign derangements in this high-risk patient population. Propofol, commonly used in TIVA, can decrease blood pressure, heart rate, cardiac output, and cardiac contractility. Sevoflurane, commonly used in inhalation anesthesia, is less likely to have significant effects on cardiac output or heart rate but in high doses can cause hypotension. Fluid management and vasopressor use is critical in managing persistent hypotension intraoperatively. The 2013 guideline from the American Association of Neurological Surgeons recommends maintaining the mean arterial pressure (MAP) between 85-90 mmHg for the first 7 days after injury to improve neurological outcomes. There is some debate as to whether there is sufficient evidence for the specific MAP goal and time period to maintain this goal, but it is undeniable that hypotension is detrimental to perfusing the spinal cord and can cause further neurological devastation.13
Autonomic hyperreflexia or dysfunction is another feared complication peri-operatively and while in awake patients, this can manifest as headaches or sweating, in anesthetized patients, this will present as hypertension or bradycardia. The most severe consequence of this complication is intracerebral or subarachnoid hemorrhage.17 Some immediate interventions that the anesthesiologist can take to alleviate this response include deepening the anesthetic agent to help decrease the blood pressure and administering emergency antihypertensive medications, such as intravenous hydralazine or nitroprusside.18 There has been a case report of IV lidocaine being used to alleviate severe hypertension.19
Another option is the use of dexmedetomidine as the primary sedative agent. One case report from 2014 outlined the use of this agent in a patient with a T7 level SCI undergoing a bladder stone removal with no events of autonomic dysreflexia.20 Another case report from 2019 demonstrated the use of dexmedetomidine and fentanyl in a patient with a T11 level SCI undergoing an orchiectomy with no events of autonomic dysfunction during the case.21
Regional anesthesia may also be an option for preventing autonomic dysfunction. Spinal anesthesia has been shown in urological surgeries to help prevent the development of autonomic hyperreflexia.22 Epidural anesthesia is a safe option for pregnant SCI patients as well as those undergoing abdominal surgeries that do not require general anesthesia. Finally, for upper extremity surgeries, nerve blocks such as a brachial plexus block present a feasible option as well.23
Postoperative care
Chronic pain affects many SCI patients, with estimates ranging from 63-90% of individuals reporting some sort of chronic pain affecting their daily life. After a surgical procedure, it is logical that these individuals will experience increased pain during their recovery period. Two broad categories of pain experienced are neuropathic, associated with damage to the somatosensory system, and nociceptive, associated with damage to the musculoskeletal system and visceral pain. Post-surgical pain is often nociceptive and best managed through a multimodal approach. This includes the use of acetaminophen, non-steroidal anti-inflammatory drugs, opioids, and topical analgesics in conjunction with regional nerve blocks, physical rehabilitation, and coordination with the interventional pain management team.24
Special populations
Obstetric patients with SCI pose a unique challenge to the anesthesiologist. The most serious complication this population experiences is autonomic hyperreflexia, as described earlier. Patients with SCIs should have a pre-pregnancy evaluation with a multidisciplinary team, including maternal-fetal medicine specialists, anesthesiologists, physical and occupational therapists, pediatricians, and neonatologists. The SCI patients may deliver vaginally or via Cesarean section (C-section), and neuraxial anesthesia, such as epidural or combined spinal-epidural anesthesia is recommended for prevention of autonomic hyperreflexia, as the anesthetic will block the noxious stimuli from the reproductive organs. In a case study from 2022, a 29-year-old woman with a T6 SCI injury underwent a C-section with spinal anesthesia (low concentration ropivacaine) and dexmedetomidine for sedation and did not develop autonomic hyperreflexia.25 If a patient giving birth appears to be experiencing autonomic hyperreflexia, immediate treatment includes repositioning the patient, stopping any stimuli such as a cervical exam, relieving any obstructed catheters, and placing the patient in an upright position to allow for pooling of blood in the abdomen and lower extremities, causing a reduction in blood pressure.26 Other interventions include administration of emergency anti-hypertensive medications such as nifedipine or labetalol.
Pediatric patients with SCI also require specialized care in the pre-, peri-, and post-operative periods. Nil per os (NPO) guidelines for children vary at different institutions and some will allow for children under 6 months to be NPO for milk and solids for only 4 hours, and children between 6 months and 3 years for only 6 hours. However, SCI patients are at a higher risk for delayed gastric emptying due to a variety of factors, including pain, ileus, medications, and the SCI lesion itself. Therefore, adhering to stricter NPO guidelines such as “NPO after midnight” or “NPO for 8 hours” may be best practice in reducing the risk of aspiration.27 Premedication is sometimes offered for anxious pediatric patients prior to arriving in the OR. The most common medication offered is a benzodiazepine, often midazolam. While this may be an appropriate option, it is important to note that this may exacerbate hypotension in an already vulnerable population, so it must be offered with caution. A calming presence in the OR, such as the anesthesiologist, OR nurse, surgeon or child-life specialist is essential in caring for these patients.28
Conclusions
The SCI patients ranging from the pediatric to the geriatric population are undergoing surgery every day in the United States and anesthesiologists must take great attention in providing high-quality medical care. More research is needed in determining specific agents of anesthetics that may be tailored to the SCI population. Understanding the options that may be offered, from local nerve blocks to spinal anesthesia to general anesthesia, is critical in formulating a safe and effective anesthetic plan and requires coordination from a multidisciplinary team dedicated to providing the best care possible for these patients.