

Introduction
Acute perforation of the gallbladder a rare but life-threating complication associated with a high risk of morbidity and mortality of 12-42%.1,2 Its incidence is estimated as 2% of all gallbladder diseases and 30% of patients with acute cholecystitis.3
Obstruction of the gallbladder or cystic duct site is considered to be the initiating event in a cascade that leads to increased intraluminal gallbladder pressure, ischemia, necrosis and eventually perforation of the gallbladder wall. The most common site of perforation is the gallbladder fundus, presumably due to being the region of the gallbladder most susceptible to ischemia.2,4,5 Although acute cholecystitis is twice more common among females,6 gallbladder perforation is more frequent in males.2,7,8
Risk factors
Several risk factors for gallbladder perforation have been identified, including older age,1,2,9 male sex,1,9 presence of gallstones,1,2,9 diabetes mellitus,2,9 steroid use,10 Typhoid fever,11 malignancies,12 cirrhosis,1 immunodeficiency states or immunotherapy,1 Hispanic ethnicity,13 and cardiovascular comorbidities (hypertension, cardiac diseases, and atherosclerosis).9,13
Classification
The classification of gallbladder perforation was initially proposed by Neimeier in 193414 to include three types: chronic gallbladder perforation with fistulous formation to the surrounding structures leading to biliary-enteric fistula (Type 1), subacute perforation leading to the formation of a localized peri-cholecystic abscess (Type 2), and acute free perforation of gallbladder into the peritoneal cavity (Type 3). Unfortunately, the Niemeier’s classification continues to be erroneously cited by numerous authors who interchange Type 1 and 3.
Later on in 1987, Anderson et al15 modified the classification and added a Type 4 perforation, described as formation of a fistula between the gallbladder and the biliary tree.
This modified classification remains the most widely used classification for gallbladder perforation and is shown in Table 1.
Presentation and diagnosis
Given the typical absence of pathognomonic signs or symptoms, the clinical distinction of gallbladder perforation from acute non-perforated cholecystitis remains challenging and commonly leads to diagnostic delays. Thus, a preoperative diagnosis of perforated gallbladder is only made in 3% of patients,13 Autopsy studies of patients that died secondary to gallbladder perforation have shown that the diagnosis was not suspected in any of them.16
Presenting clinical features can range from non-specific abdominal symptoms to acute generalized peritonitis. The most common presenting symptoms are fever, jaundice, and right upper quadrant pain.1 Tachycardia, generalized peritonitis, and septic shock can also be present in severe cases.9 In patients initially presumed to have acute non-perforated cholecystitis, perforation of the gallbladder should be suspected in patients with high fever, leukocytosis, rise in liver enzymes, and rapid clinical deterioration.
Each type of gallbladder perforation may have some unique clinical features. Type 1 (acute free perforation) may be associated with signs of generalized peritonitis, whereas Type 2 (subacute pericholecystic abscess) can present with localized peritonitis in the right upper quadrant. Type 3 (chronic fistulation to the surrounding structures) can show signs that are specific to the sites of fistulation: gallstone ileus or recurrent attacks of cholecystitis and cholangitis in cases of a cholecysto-enteric fistula,17 persistent effusions in cholecysto-pleural fistula,18 symptoms of liver abscess and septic thrombophlebitis with intra-hepatic gallbladder perforations,19 or signs of intra-muscular abscess when perforating into the abdominal wall.20 Type 4 (cholecysto-biliary fistula) can present with a longstanding history of gallstones, signs of acute or chronic cholecystitis, and jaundice.21
Given the lack of characteristic clinical features and laboratory values to distinguish between non-perforated cholecystitis and gallbladder perforation, imaging studies are crucial for preventing further diagnostic and treatment delays.
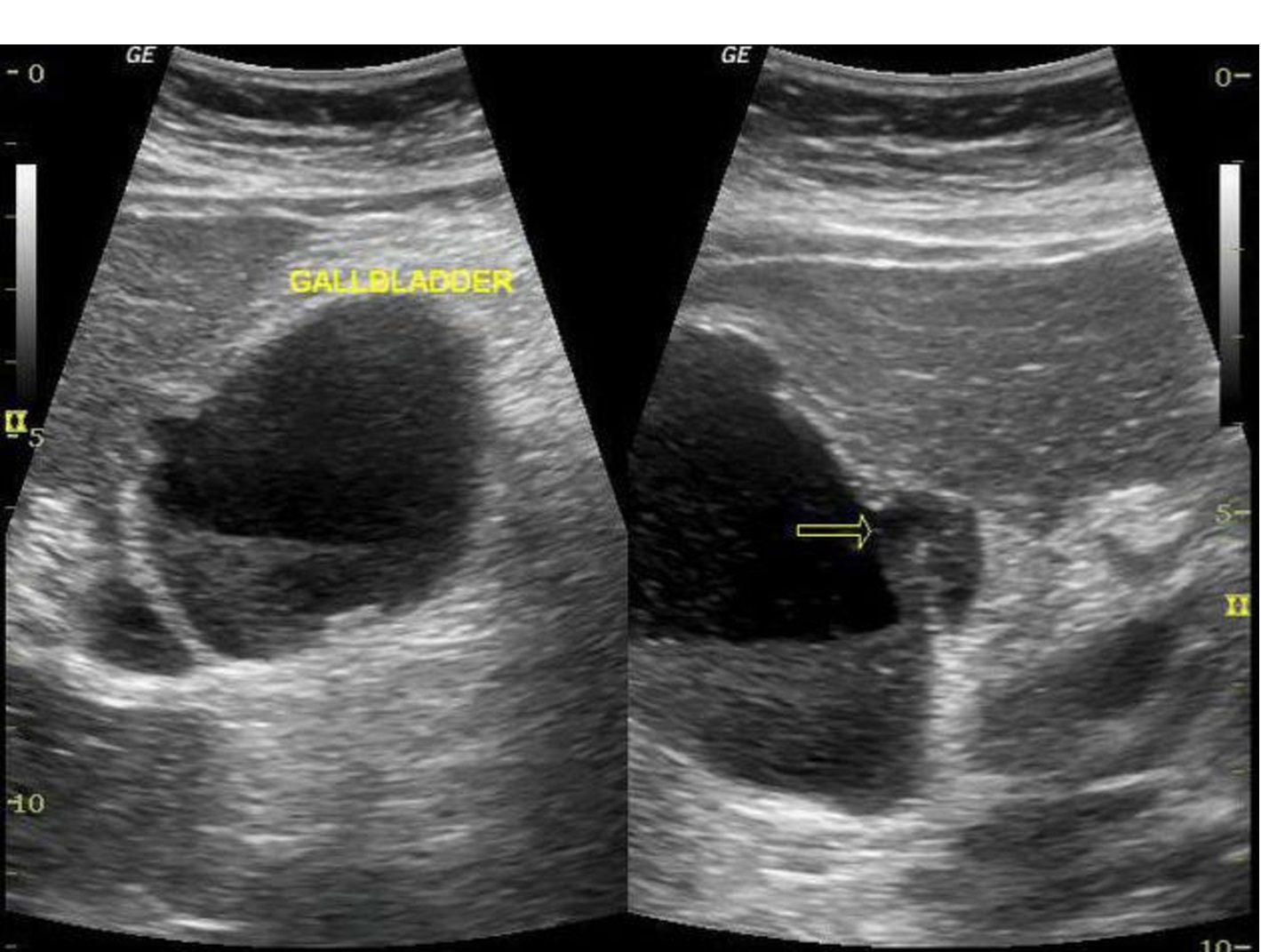
However, selection of appropriate imaging modalities is very important. Abdominal X-ray is of little value, although in some cases of Type 3 (cholecysto-enteric fistula) can show enteric air-fluid levels and an opaque intra-luminal gallstone suggestive of a gallstone ileus.2 Although abdominal ultrasound (US) it the most common imaging study obtained in patients presenting with biliary symptoms, in most cases yields signs of acute cholecystitis (gallbladder wall thickening and pericholecystic fluid) and gallstones. In cases Type 1 (acute free perforation) abdominal US can show intraperitoneal free fluid in patients.2 The sonographic ‘hole sign’ (a defect in the gallbladder wall)22 (Figure 1), is the only specific sign of gallbladder perforation. However, although some authors23 report detecting a “hole sign” in 70% of cases, many others have not been able to visualize the site of defect in any patients with gallbladder perforation.24

A contrast-enhanced CT scan of the abdomen is more sensitive and the study of choice when gallbladder perforation is suspected. The sensitivity of CT scan has been shown to 69.2%, significantly superior to that of the US (38.5%).24
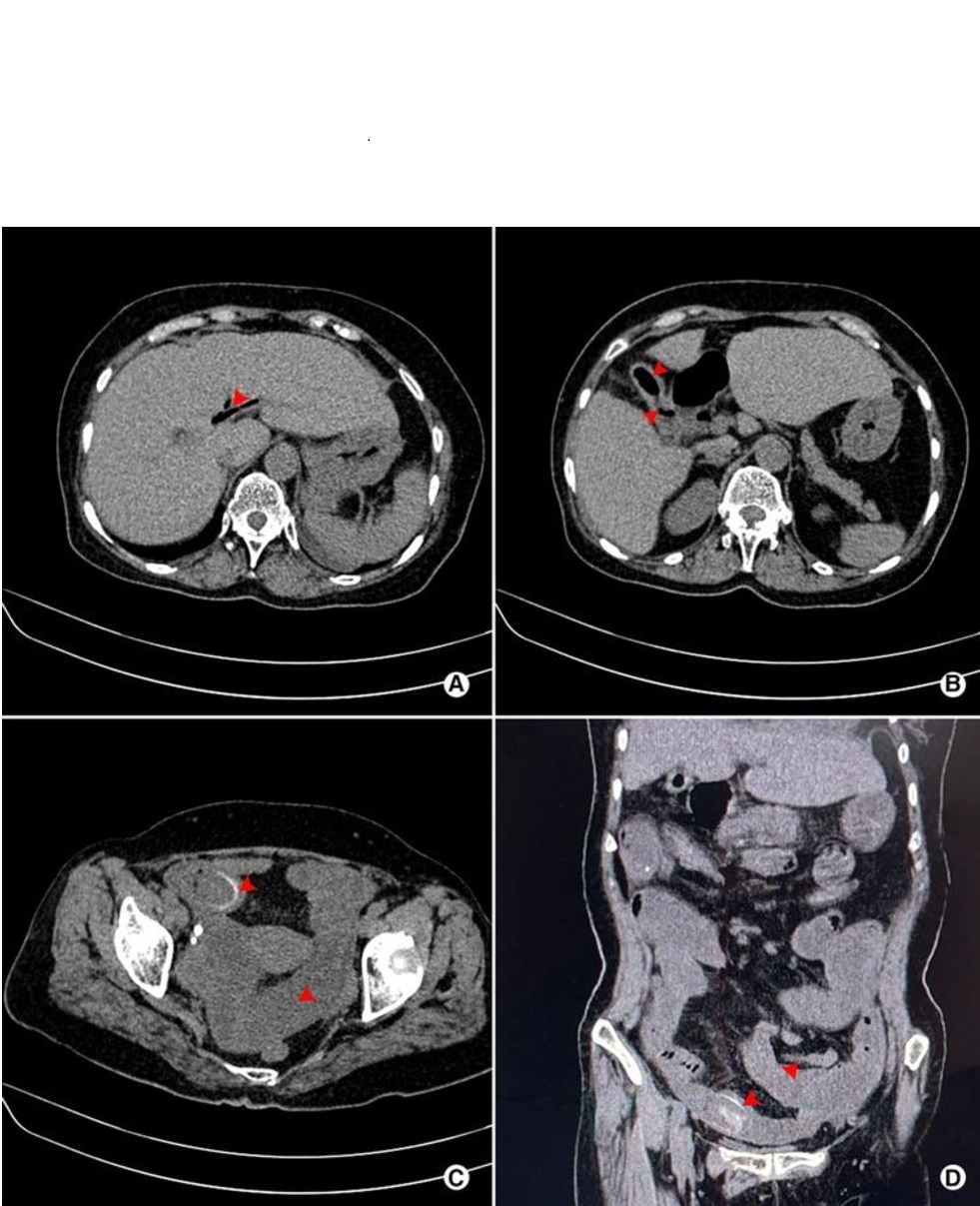
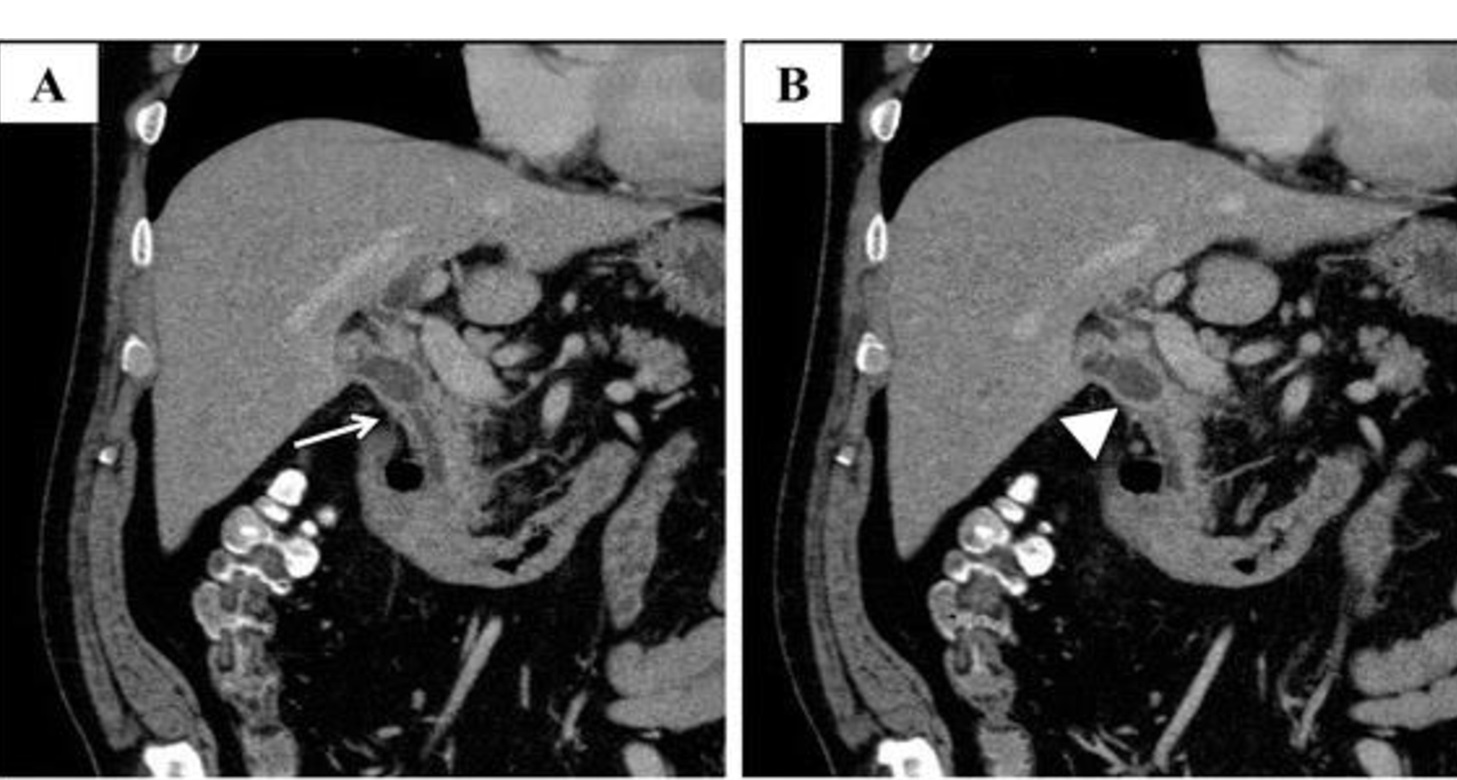
Each type of gallbladder perforation has some characteristic CT findings: presence of extraluminal gallstones, or free peritoneal fluid and/or a defect in the gallbladder wall in Type 1 perforation (Figure 2); pericholecystic stranding and abscess in Type 2 perforation (Figure 3); and pneumobilia, fistulous connection between the gallbladder, or a calcified rim-calcified gallstone impacted in the small bowel combined with dilatation of proximal small bowel in Type 3 perforation (Figure 4). Although in cholecysto-biliary fistulae (Type 4 perforation), the CT scan can show dilation of the common bile duct and an atrophic gallbladder that is coalesced with the bile ducts (Figure 5), magnetic resonance cholangiopancreatography (MRCP) is the preferred imaging study of choice for a more accurate diagnosis and delineation of the fistula anatomy.25
_and_a_defect_in_the_gallbladder_w.jpeg)
.___adopted_from_bell__324255.jpeg)
_pneumobilia_(arrow)__(b)_pneumo-gallbladder_and_ill-defined_borderlin.jpeg)
_mild_dilation_of_the_common_bile_duct_(arrow)__(b)_contracted_gallbla.jpeg)
Other imaging modalities include a hepatobiliary iminodiacetic acid (HIDA) scan that can be helpful in cases where gallbladder perforation is suspected but not confirmed by other imaging studies. In those circumstances, the HIDA scan can show a defect in the wall of gallbladder and extravasation of radioactive dye in the peritoneal cavity.2 Endoscopic retrograde cholangiopancreatography (ERCP) can also be particularly useful for localizing gallbladder fistulae in Type 3 and Type 4 gallbladder perforations.
Treatment
Treatment options for gallbladder perforation (Table 2) take into consideration the type of perforation, patient’s clinical status and estimated surgical risk, as well as the surgical expertise available.
Type 1 (acute free perforation) requires emergent surgical intervention, with a laparoscopic or open cholecystectomy with the goal of completely removing the gallbladder; however, a subtotal cholecystectomy is recommended when establishing the critical view of Calot’s safety triangle is not safe or possible. The rate of conversion to open from laparoscopy is reported to be as high as 75%,13 suggesting that the laparoscopic approach, while preferrable, can be challenging in the presence of a gallbladder perforation likely due to significant degree of gallbladder inflammation. Intra-operative closed drainage of the gallbladder fossa and post-operative antibiotic therapy could help reducing the risk of deep surgical site infections.
The management of localized (Type 2) gallbladder perforation is debated, with options including conservative management with percutaneous catheter drainage of the gallbladder and antibiotics followed by interval cholecystectomy; immediate cholecystectomy and washout of the local abscess; or only percutaneous catheter drainage of the gallbladder and subhepatic abscess and antibiotics in high- risk surgical patients or those refusing surgery.1,2,28,29 Follow-up study of patients treated with percutaneous catheter drainage alone, show that 70% of them did not experience recurrent cholecystitis and did not require any further interventions after interval removal of the catheter.29
A cholecysto-enteric fistula (Type 3 gallbladder perforation) without gallstone ileus are usually treated with closure the fistula tract (suturing, stapling, or omental flap coverage) and cholecystectomy.30 In some cases, complete fistula resection and reconstruction may be necessary, such as a Billroth-2 gastrojejunostomy in cases of a fistula between the gallbladder and the duodenum.30
In patients with gallstone ileus,31 options include:
-
Enterolithotomy alone via a simple vertical enterotomy to remove the gallstone followed by closure of the enterotomy transversally.
-
Enterolithotomy, cholecystectomy, and closure the fistula tract (one-stage procedure)
-
Enterolithotomy with cholecystectomy + delayed fistula repair (two-stage procedure)
However, in the presence of severe inflammation and adhesions, removal of the stone alone and not addressing the fistula and gallbladder is advised particularly in elderly and comorbid patients. One-stage procedure can be performed under favorable conditions, whereas a two-stage procedure is uncommon and only considered when fistula symptoms persist.
Type 4 (cholecysto-biliary fistula) perforations are usually managed with delayed surgical management. Imaging studies to delineate the fistula location and anatomy as well as referral to a center with hepato-biliary surgery expertise are important in managing these complex fistulae. In most of these cases only a subtotal cholecystectomy is performed because a complete removal of the gallbladder not only is not absolutely necessary, but it might also not be safe or possible given the presence of dense adhesions and severe inflammation in the region of the hepatoduodenal ligament.32 Surgical options include partial cholecystectomy and using part of the infundibular to close the bile duct (infundibular diverticulization); cholecystectomy and bile duct reconstruction over T-tube; or cholecystectomy, complete resection of the fistula, and hepaticojejunostomy.32
Conclusions
Gallbladder perforation is an uncommon but challenging complication of acute cholecystitis. The lack of early and specific clinical signs and symptoms, laboratory findings, and imaging features lead to diagnostic and treatment delays that result in increased morbidity and mortality. Awareness of the risk factors associated with gallbladder perforation, a high index of suspicion, and appropriate selection of imaging modalities are crucial for timely diagnosis and treatment. Selecting the optimal treatment option for gallbladder perforation should take into consideration the type of perforation, patient’s clinical status and estimated surgical risk, as well as the surgical expertise available.