Introduction
Gastro-intestinal contrast studies with water-soluble Gastrografin are favored over a barium study due to the risk of barium-associated peritonitis in cases of perforation or leakage into the peritoneal cavity. While Gastrografin is easily absorbed by the peritoneum without causing peritonitis, given its hypertonicity, it can cause inflammation and irritation of the gastro-intestinal mucosa.1 Due to this quality of Gastrografin, it is recommended to be diluted prior to gastro-intestinal administration. In one reported case, Gastrografin given in a patient with small bowel obstruction caused hemorrhagic gastritis.2
We report a unique case of a severe acute colitis following retention of undiluted Gastrografin administered for a colonography, that was successfully managed without surgery.
Case Description
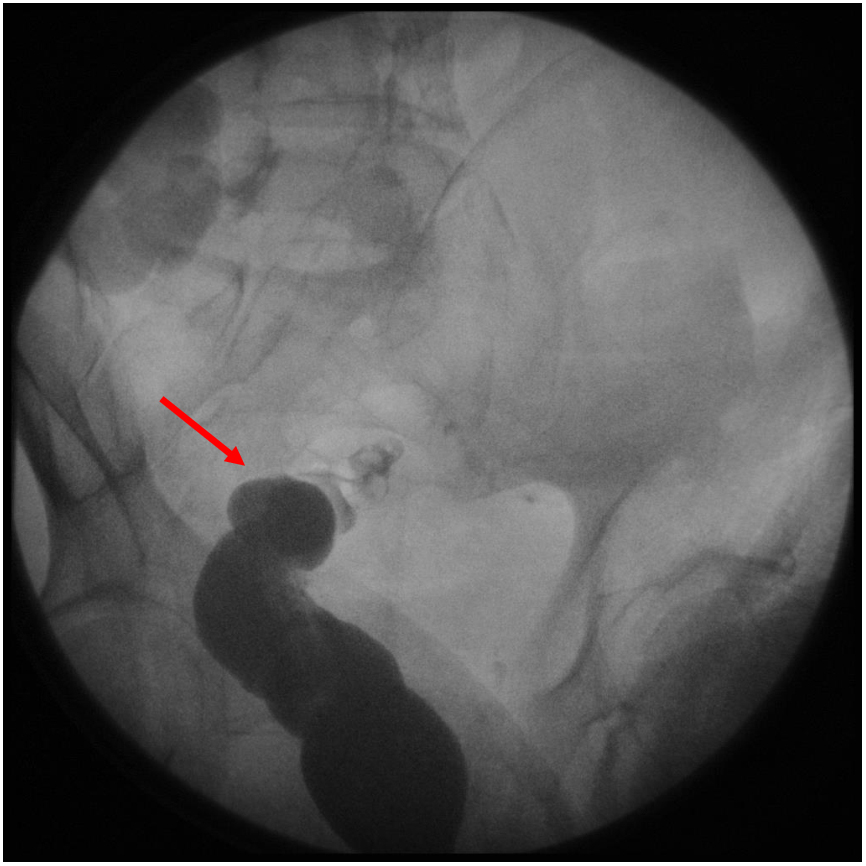
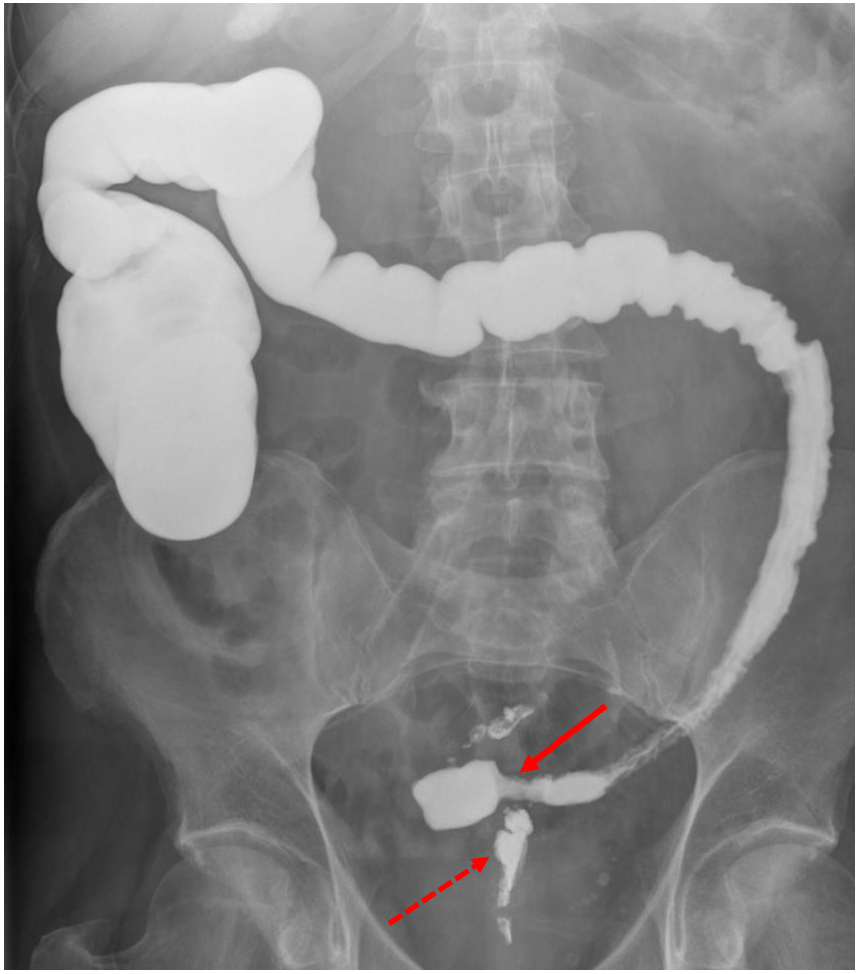
Our patient is a 57-year-old male with multiple comorbidities that included perforated sigmoid diverticulitis for which he underwent an open sigmoid resection and creation of an end-colostomy and a Hartmann’s pouch. Six years later he underwent an open colostomy takedown, left colectomy, creation of a new stapled colorectal anastomosis, and a diverting loop ileostomy. Six months after creation of his ileostomy, we started planning for the takedown of the ileostomy. As part of the pre-operative work-up we obtained a fluoroscopic barium enema study to evaluate the patency and the integrity of the colorectal anastomosis. While the study revealed no anastomotic leak, we were not able to visualize the barium traversing the anastomosis, raising concerns for an anastomotic stricture (Figure 1). To further investigate the anatomy and the patency of the anastomosis, patient underwent an antegrade, fluoroscopic Gastrografin contrast study through the distal, defunctionalized opening of the loop ileostomy, that showed a complete stricture of the colorectal anastomosis (Figure 2).


Immediately after the study, patient developed severe abdominal spasms and diaphoresis. On physical examination of the abdomen patient had severe tenderness across the entire abdomen. He was afebrile, normotensive, with sinus tachycardia. His lactic acid level was 2.3 mmol/L (normal range 0.5 – 1.8) and the white blood cell count was 22.1 K/cmm (normal range 4.5 – 10.0). The remainder of the blood counts and chemistry were normal. Administration of intravenous fluids and empiric, broad spectrum antibiotics was initiated in the surgical intensive care unit.
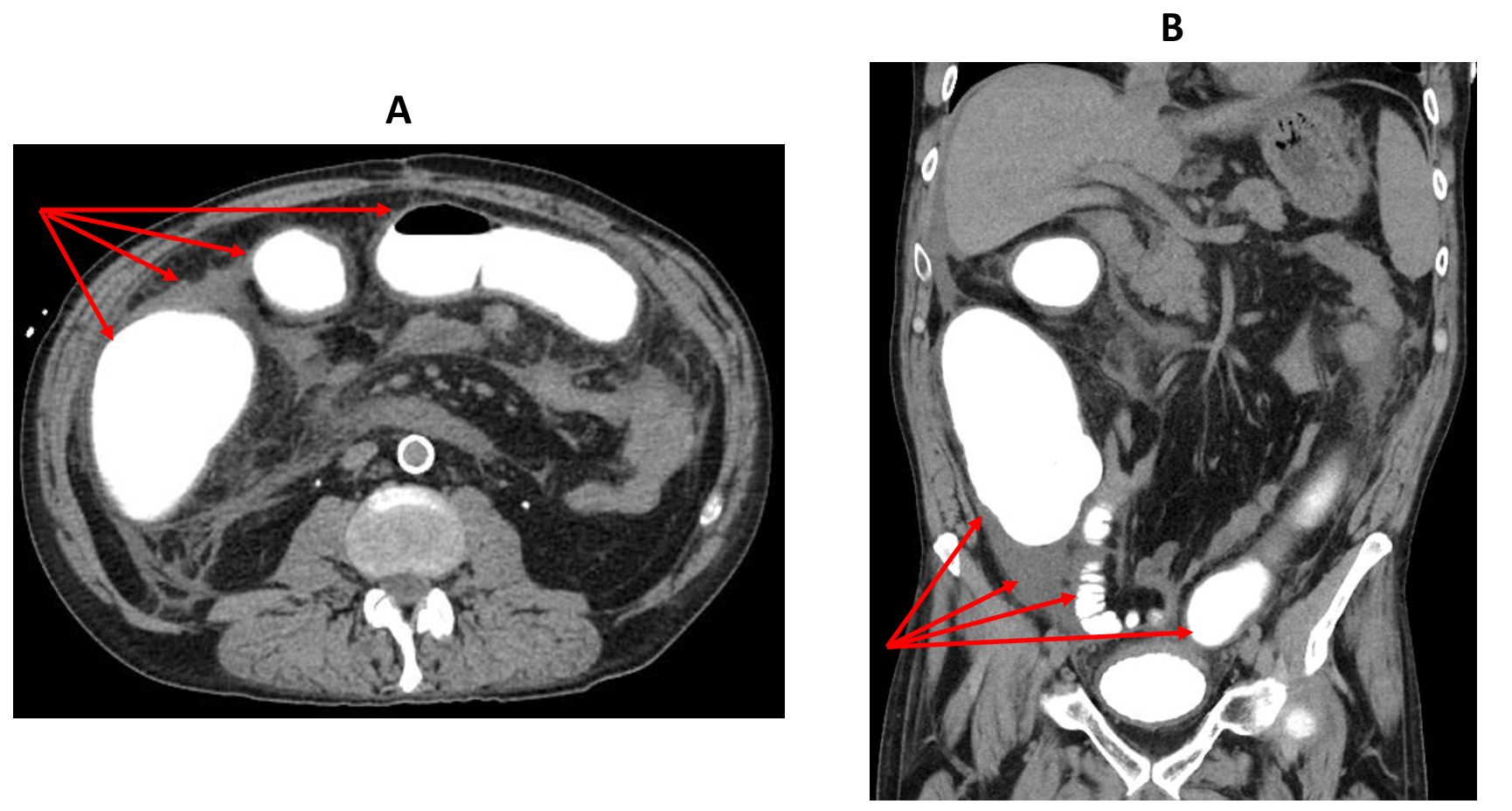
A computed tomography (CT) scan of the abdomen with intravenous contrast was obtained and showed retained Gastrografin contrast in the colon, no presence of contrast in the rectum, wall-thickening of the entire colon (most intensely in the ascending colon), pericolonic stranding and free fluid, and wall thickening of the distal ileum (Figure 3). These findings were suggestive of a stricture of the colorectal anastomosis, colitis, and distal ileitis.
_and_coronal_(b)_ct_scan_of_the_abdomen_showing_wall_thickening_of_the_entire_col.png)
Given the sudden onset of the patient’s symptoms after administration of the Gastrografin through the distal ileum, the Gastrographin administration protocol was reviewed by the radiology team. An error was identified in the administration of undiluted Gastrografin (300-500ml), instead of the usual diluted solution. This iatrogenic error was immediately disclosed to the patient and his family members.
The management of this complication was discussed in a multidisciplinary fashion involving the patient, his family members, and the General Surgery, Interventional Radiology, and Gastroenterology teams. Given the inability of the retained colonic contrast to pass into the rectum due to an anastomotic stricture, and concerns for progression of colitis with ischemia and perforation, patient underwent an urgent endoscopy via the distal, defunctionalized ileostomy opening. The retained distal ileal and colonic Gastrografin was successfully suctioned endoscopically. The patient quickly improved afterwards with resolution of his abdominal pain, tolerating a regular diet and having a productive ileostomy.
Three days later, he started passing large volume discharge from the rectum, suggesting some restoration of anastomotic patency. However, an attempt at over-a-wire colonoscopic dilation of the strictured colorectal anastomosis was not successful as not even the wire could traverse the anastomosis. The remainder of the hospital stay was uneventful. He was discharged to home after a 10-day stay in the hospital and has been doing well on a subsequent follow-up visit, with plans for an interval surgical revision of the colorectal anastomosis and ileostomy takedown.
Discussion
To the best of our knowledge, this is the first report of severe colitis following intra-colonic retention of Gastrografin.
According to professional product information,3 Gastrografin is a hyperosmolar water-soluble contrast media that contains a mixture of sodium amidotrizoate and meglumine amidotrizoate in a proportion of 10:66. Its osmolarity is about 1900 mOsm/L, which is about 6 times that of the extracellular compartment. Gastrografin is considered inferior to barium sulphate in visualizing the gastrointestinal mucosa but is preferred if there is risk of peritoneal contamination due to its solubility in water and decreased risk of subsequent peritonitis. It can be administered orally by drinking the diluted solution or introduced as an enema through the rectum.
Side effects associated with Gastrografin use are usually mild to moderate and transient in nature. Vomiting, nausea, and diarrhea are the most frequent side effects. However, severe and life-threatening reactions (anaphylactoid and hypersensitivity reactions, hyperthyroidism, tachycardia, cardiac arrest, shock hypotension, bronchospasm, toxic epidermal necrolysis) as well as deaths have been reported. For colonic studies, Gastrografin (100 ml) is usually diluted with water for a total volume of 500 ml.
In cases of prolonged retention of Gastrografin in the gastrointestinal tract (such as obstruction or stasis), tissue damage, bleeding, bowel necrosis and intestinal perforation may occur, although very rarely (<1/1000).
Lutzger et al,4 studied the effects of Gastrografin in rat colonic mucosa and found that it was associated with mucosal changes that ranged from mild to severe. Mild changes included lamina propria edema, acute mucosal inflammation and congestion, and swelling of individual gland cells. The severe alterations included mucosal atrophy, diffuse edema and acute inflammatory
cell infiltrate in the lamina propria, focal and more extensive mucosal necrosis, and transmural necrosis with acute peritonitis. The degree of inflammatory changes caused by Gastrografin was significantly higher that saline or barium sulfate.
In our patient, Gastrografin was administered undiluted and was retained in the colon due to a complete distal obstruction at the level of colorectal anastomosis. This led to severe acute inflammation of the colonic wall that could have led to colonic perforation if the Gastrografin was not evacuated endoscopically.
Our experience highlights the importance of awareness of Gastrografin complications, administration of diluted Gastrografin for colonic imaging studies, avoidance of Gastrografin use when colonic obstruction is suspected, and the urgency of evacuating Gastrografin retained in an obstructed colon.
When faced with Gastrografin-induced colitis, evaluation and management by the gastroenterology, radiology, and surgery teams in a multidisciplinary fashion is crucial. Based on our experience, we advocate for an attempt at endoscopic removal of the retained Gastrografin as the first step, in parallel with fluid resuscitation and intravenous empiric antibiotics. If endoscopic Gastrografin removal is not feasible or successful and the patient clinical condition worsens, a prompt surgical exploration should be considered to remove the retained Gastrografin via a colotomy, colostomy, or distal ileostomy with on-table endoscopy, and manage colonic ischemia and necrosis if present.
Conclusions
Gastrografin-induced colitis is a very rare but serious complication that could lead to necrosis and perforation. Radiologists and surgeons should remain vigilant about patient selection for a colonography, avoiding Gastrografin when complete bowel obstruction is suspected, the correct use of Gastrografin, and its possible complications. A multidisciplinary management approach involving the gastroenterology, radiology, and surgery teams is important in successfully treating Gastrografin-induced colitis.
Disclosure Statement
The authors have no conflicts of interest or financial disclosures to declare.